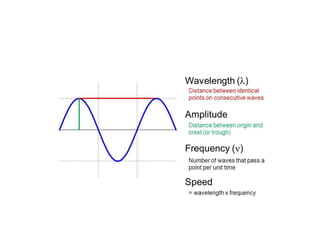
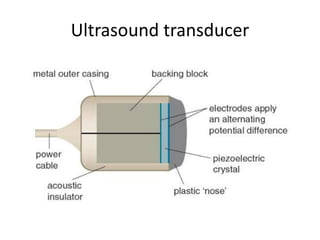
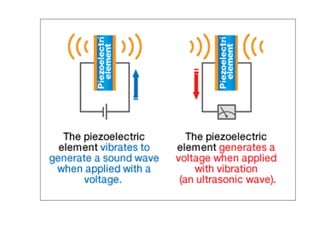
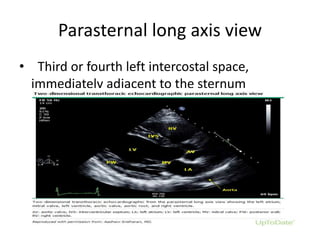
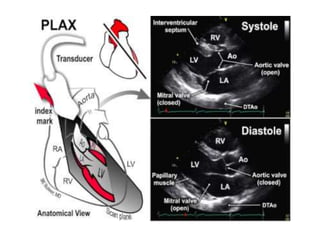
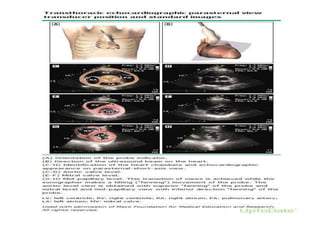
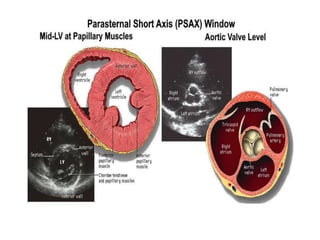
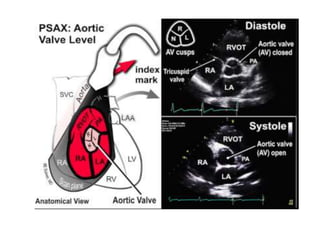
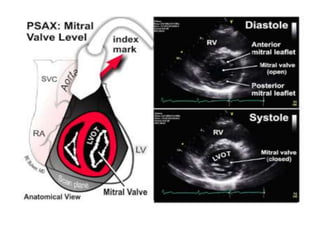
2D echocardiography uses ultrasound waves between 1-20 MHz to generate images of the heart. Ultrasound transducers use piezoelectric crystals to generate and receive ultrasound waves, and different views of the heart are obtained by manipulating the transducer position and orientation. Standard views include the parasternal long and short axis, apical 4-chamber, subcostal, and suprasternal views, which allow visualization of the heart structures and assessment of wall motion.