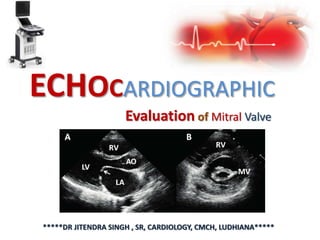
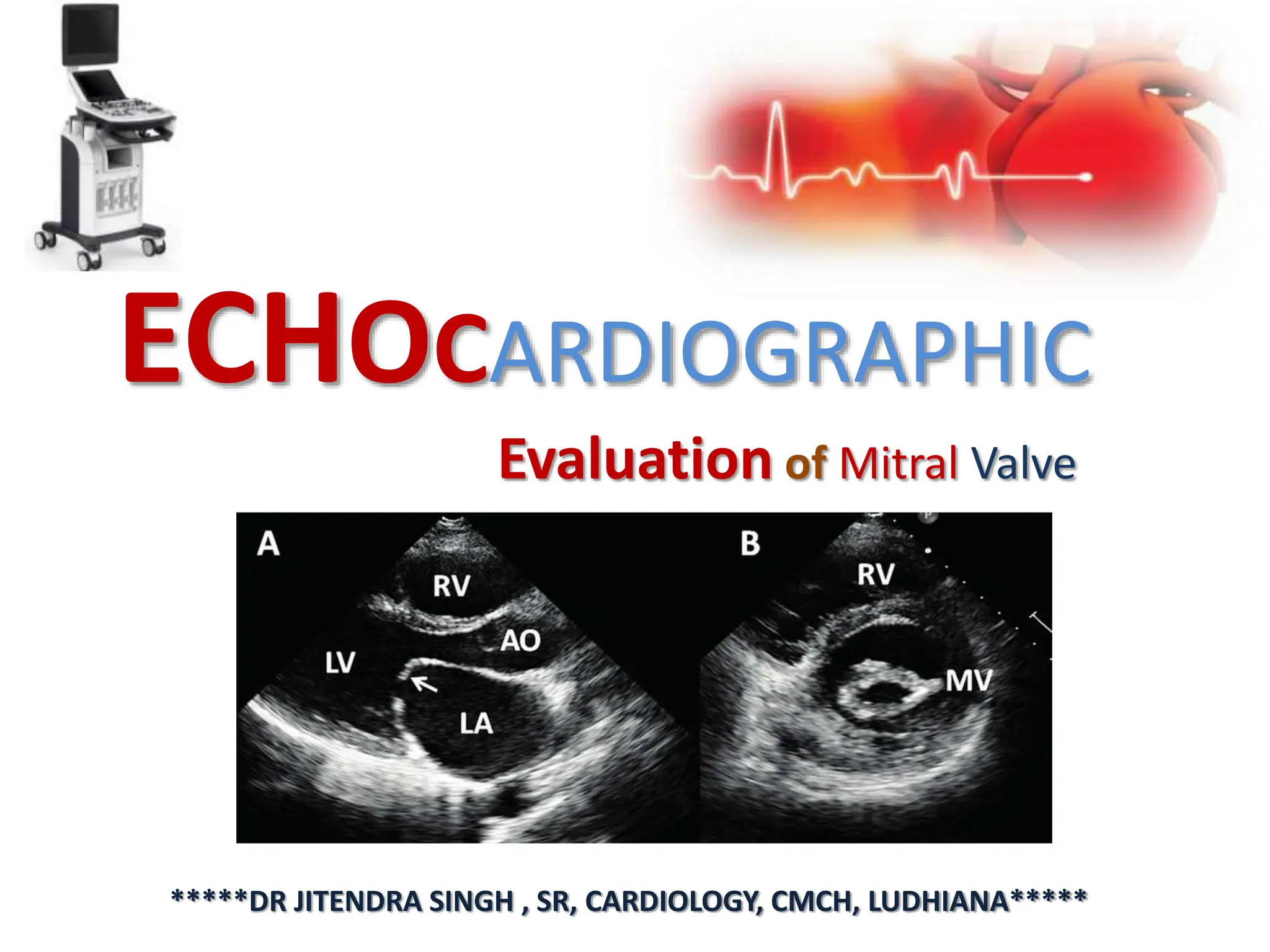
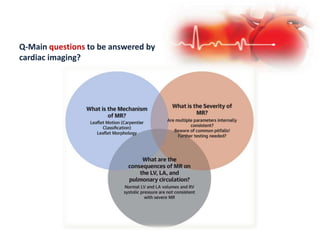
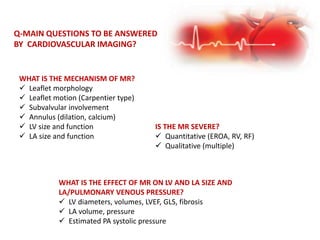
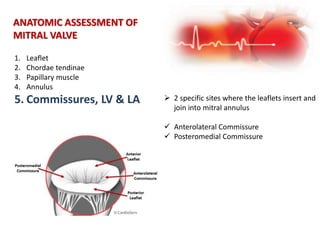
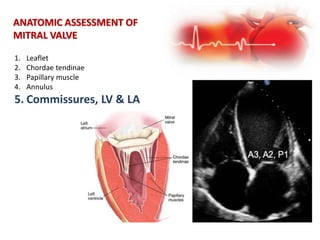
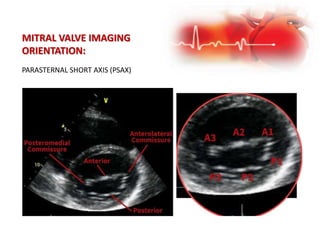
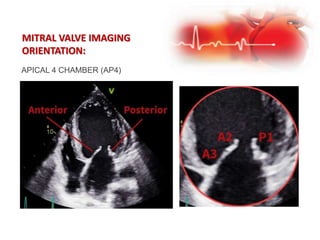
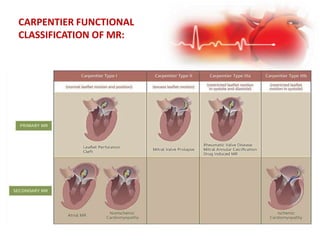
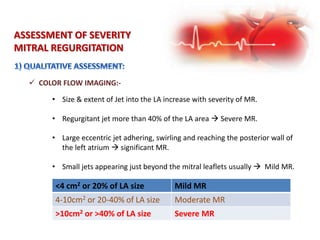
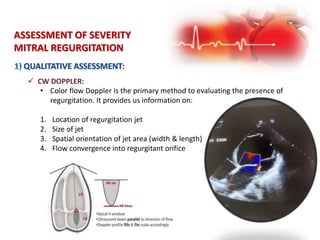
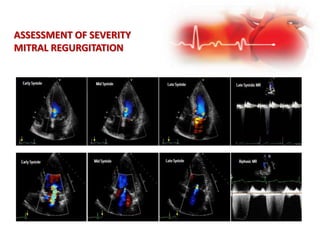
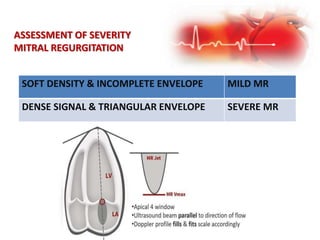
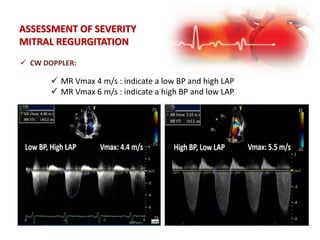
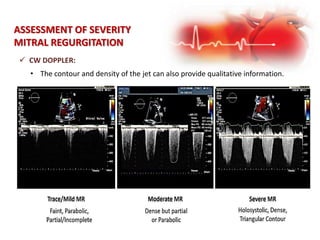
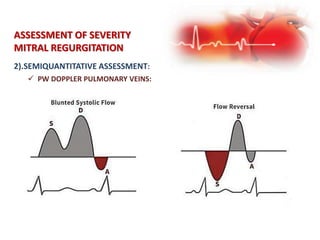
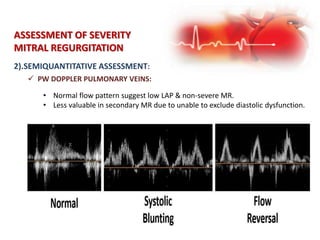
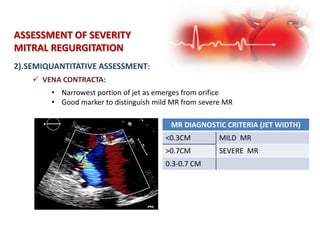
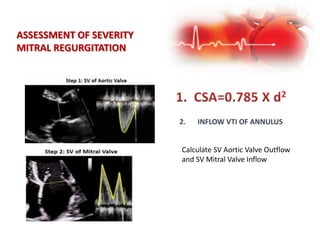
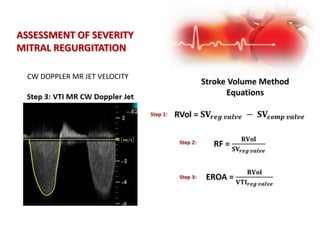
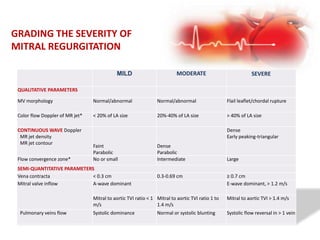
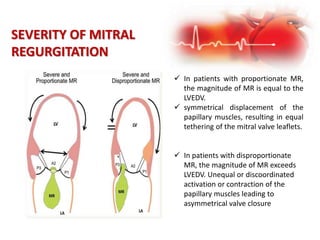
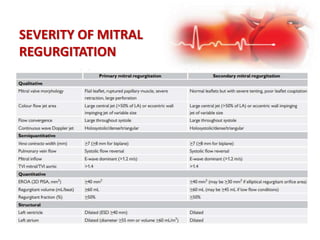
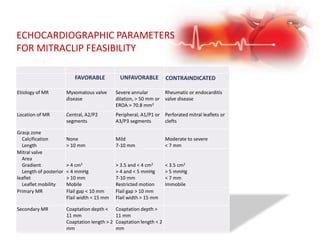
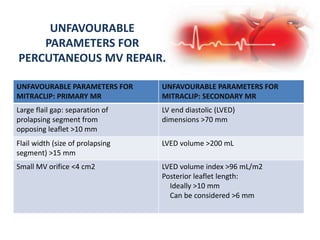
Echocardiography is used to evaluate the mitral valve and assess mitral regurgitation (MR). Key questions addressed include the mechanism of MR, severity of MR, and impact on heart structures. Severity is determined semiquantitatively by measuring jet size, density, and width of the vena contracta, as well as assessing pulmonary vein flow. Leaflet morphology, motion, chordae, annulus, and left ventricular size and function are evaluated to identify the etiology and type of MR based on the Carpentier classification system. Anatomic features are also assessed for surgical or transcatheter treatment options.