Download to read offline

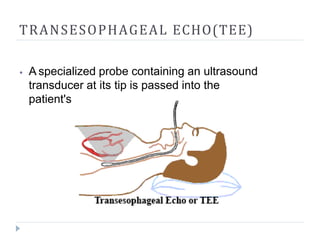

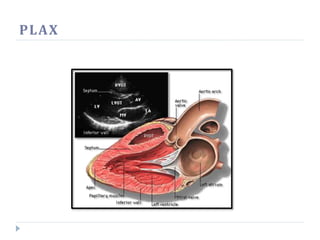


Echocardiography uses ultrasound to create images of the heart. The main types are transthoracic and transesophageal echocardiograms. Transthoracic echocardiograms place the probe on the chest to view heart structures, while transesophageal echocardiograms pass a probe into the esophagus for clearer images. Echocardiography can identify issues like blood clots, fluid around the heart, valve problems, and cardiomyopathies. Standard views obtained are parasternal long and short axis, apical 4-chamber, and subcostal. Doppler echocardiography assesses blood flow velocities.
























































