
Downloaded 166 times


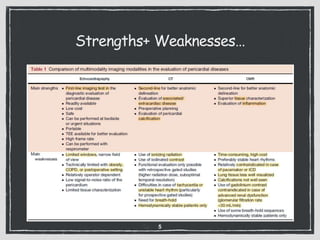
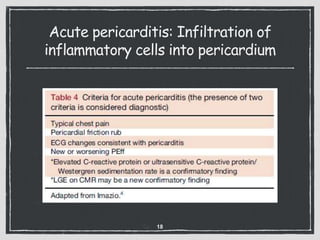
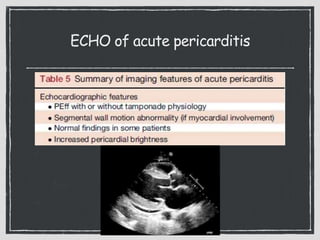
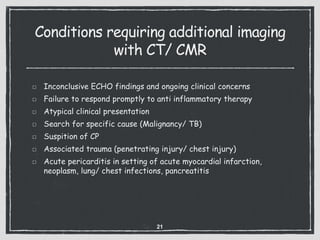

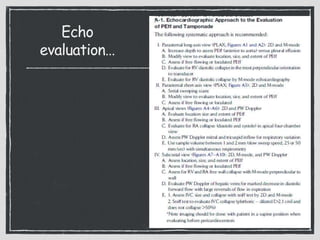
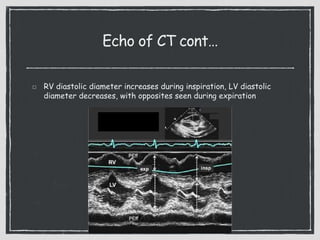
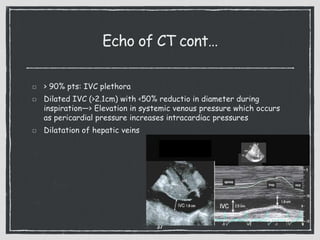


This document provides an overview of echocardiography in pericardial diseases. It begins with an introduction to pericardial anatomy and pathophysiology. It then discusses various pericardial diseases that can be evaluated by echocardiography, including acute pericarditis, recurrent pericarditis, pericardial effusions, cardiac tamponade, and constrictive pericarditis. For each condition, it describes the echocardiographic findings and techniques used to evaluate the condition. It emphasizes that echocardiography is usually the initial imaging test of choice but that CT or CMR may be needed in some complex cases.























































































