Downloaded 1,836 times
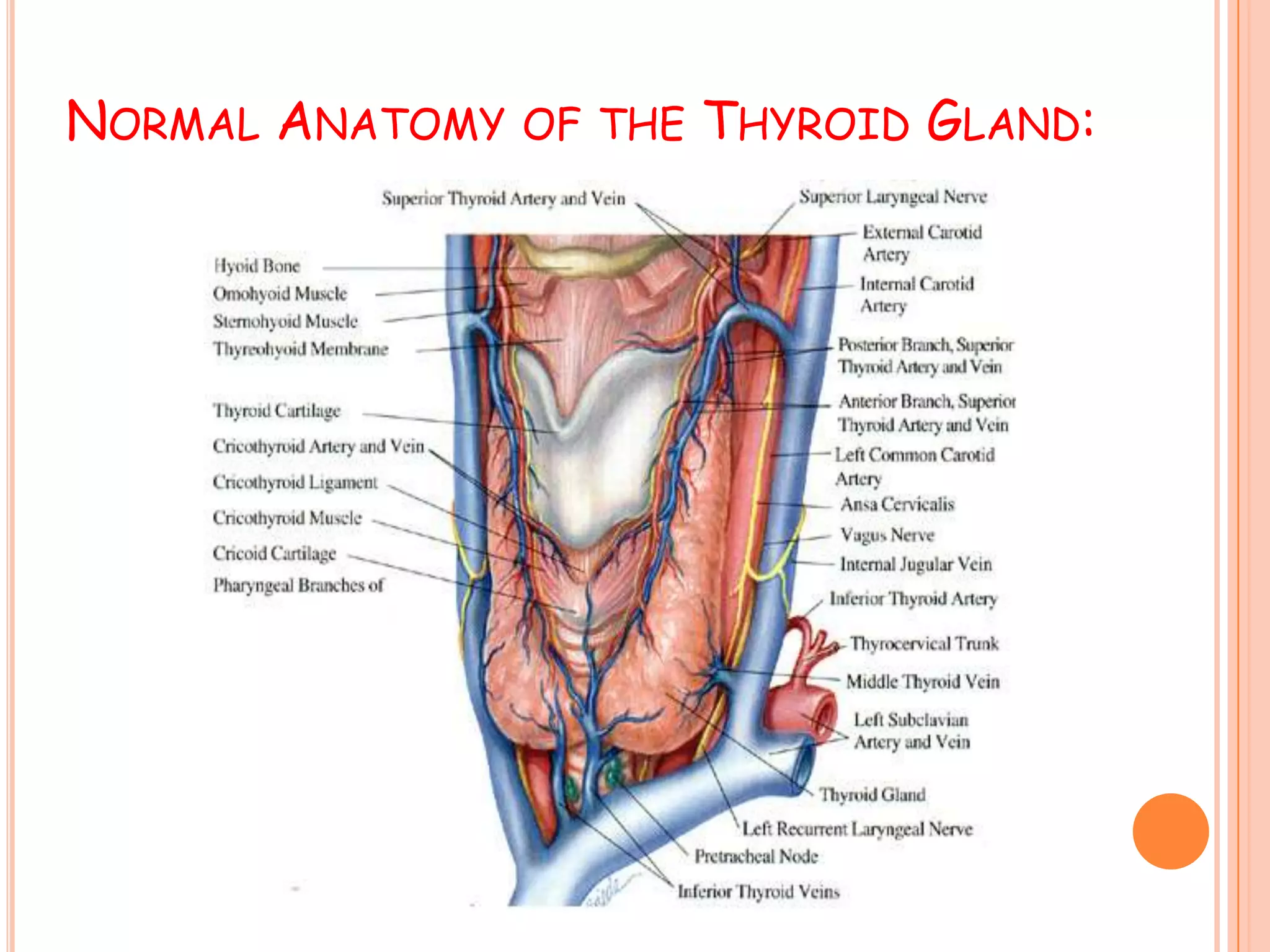
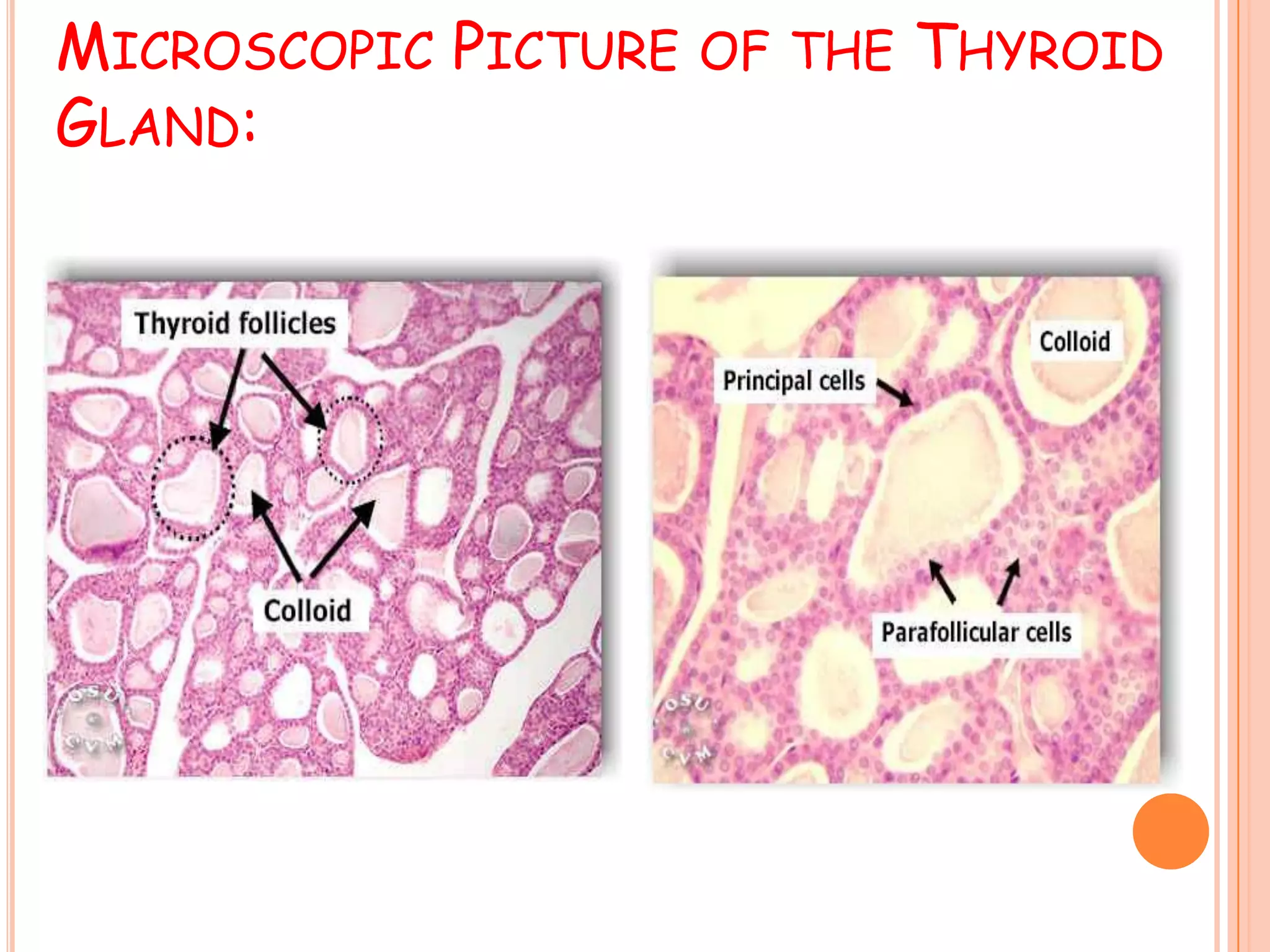
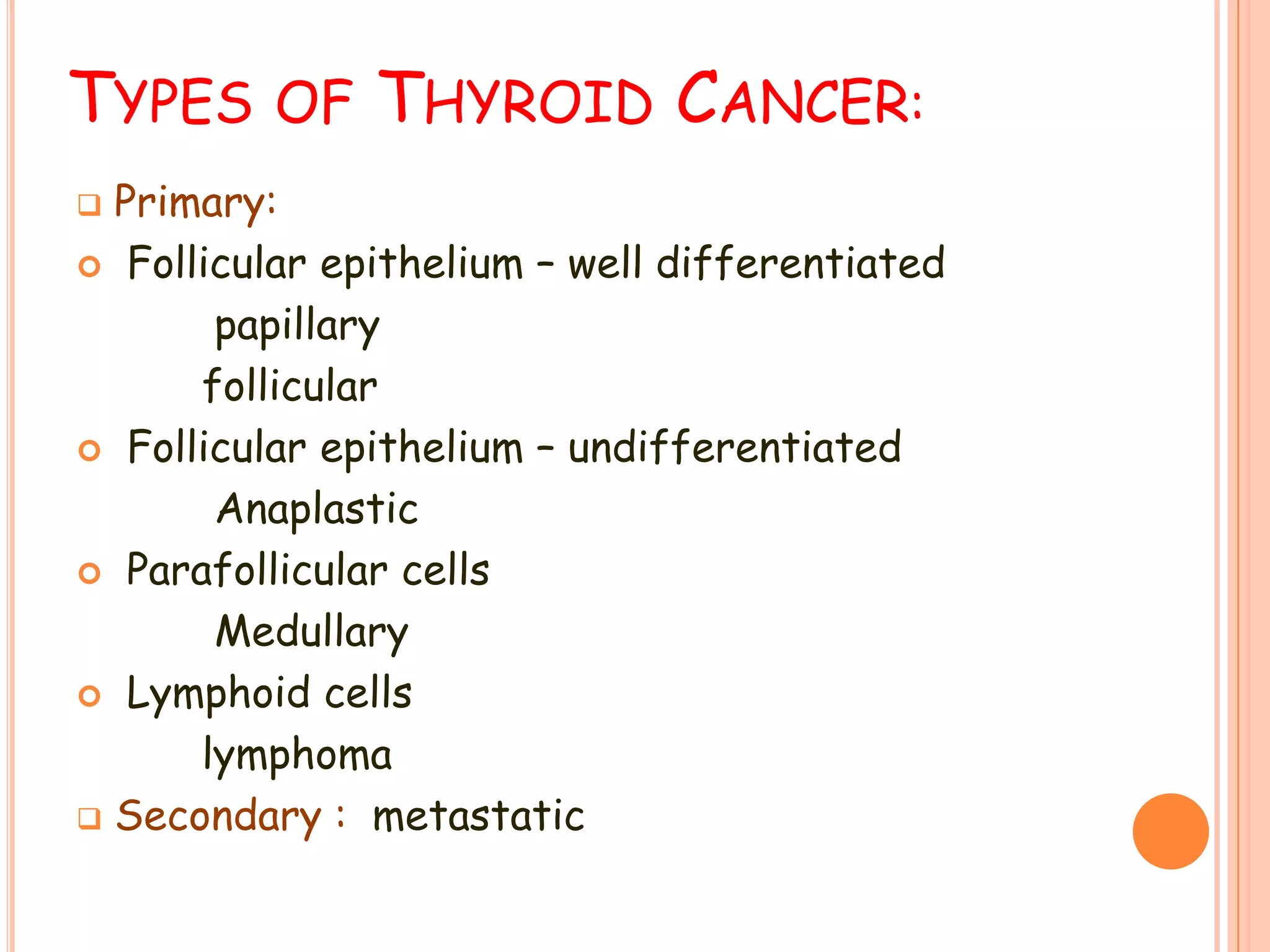
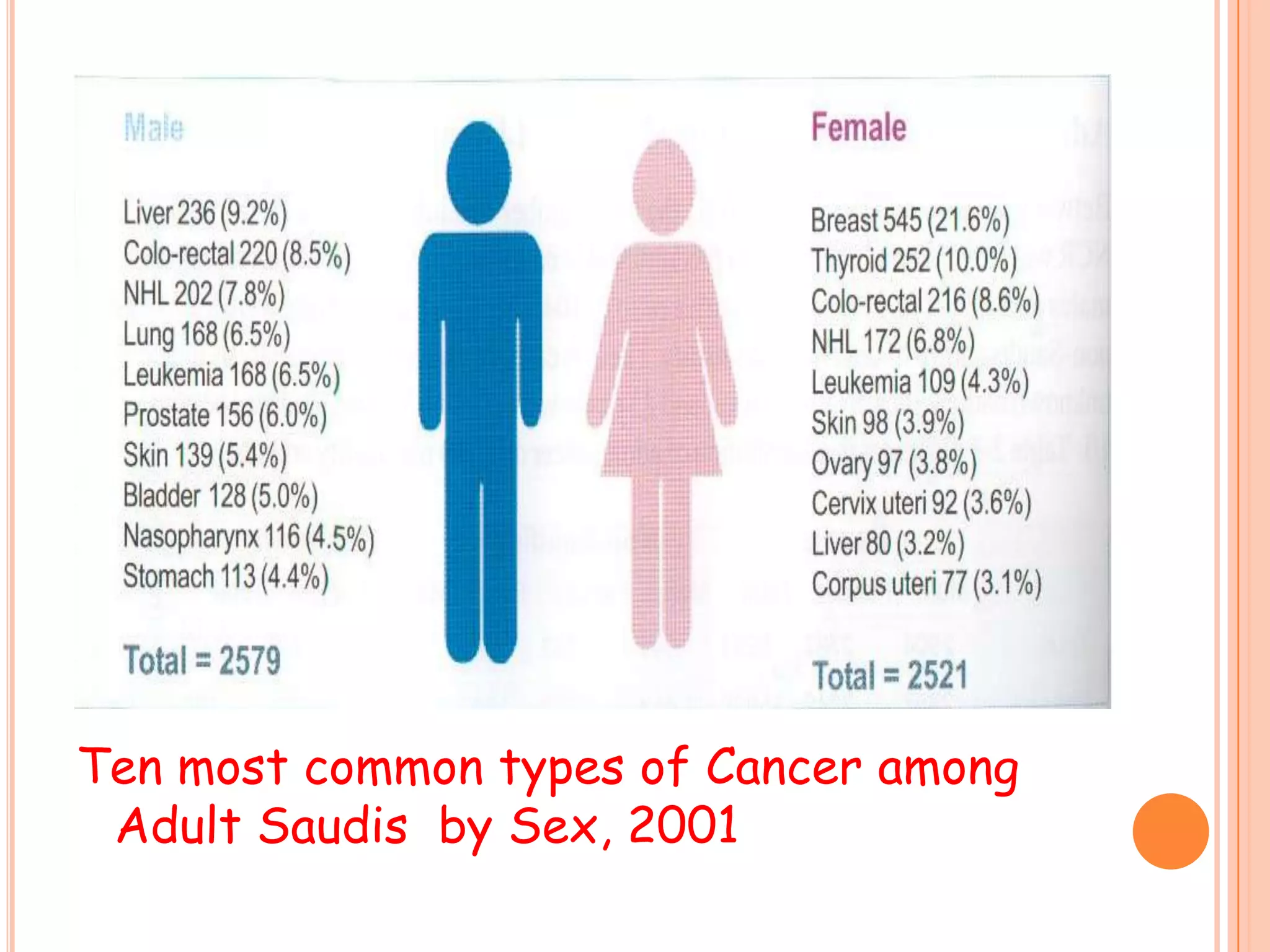
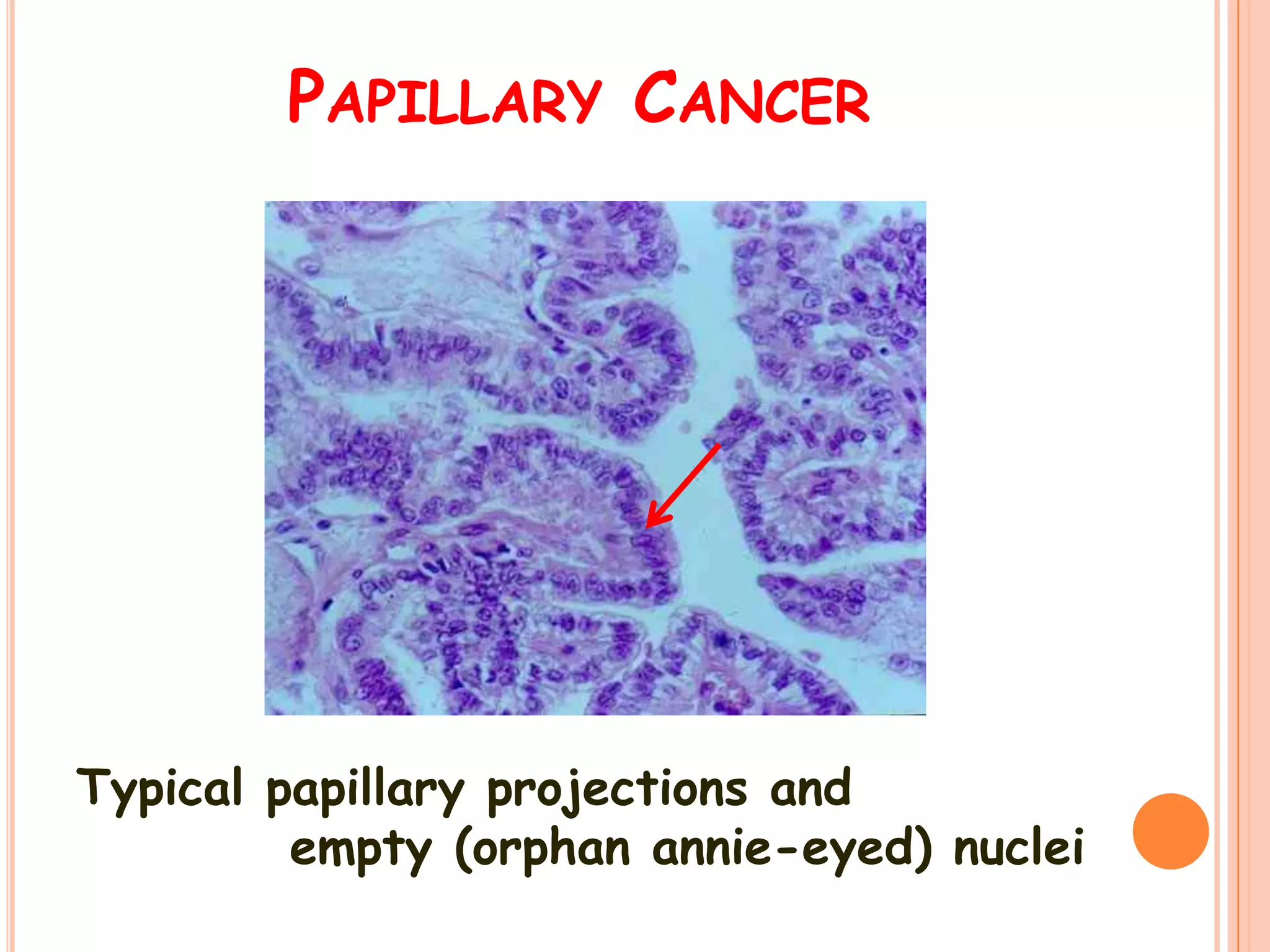
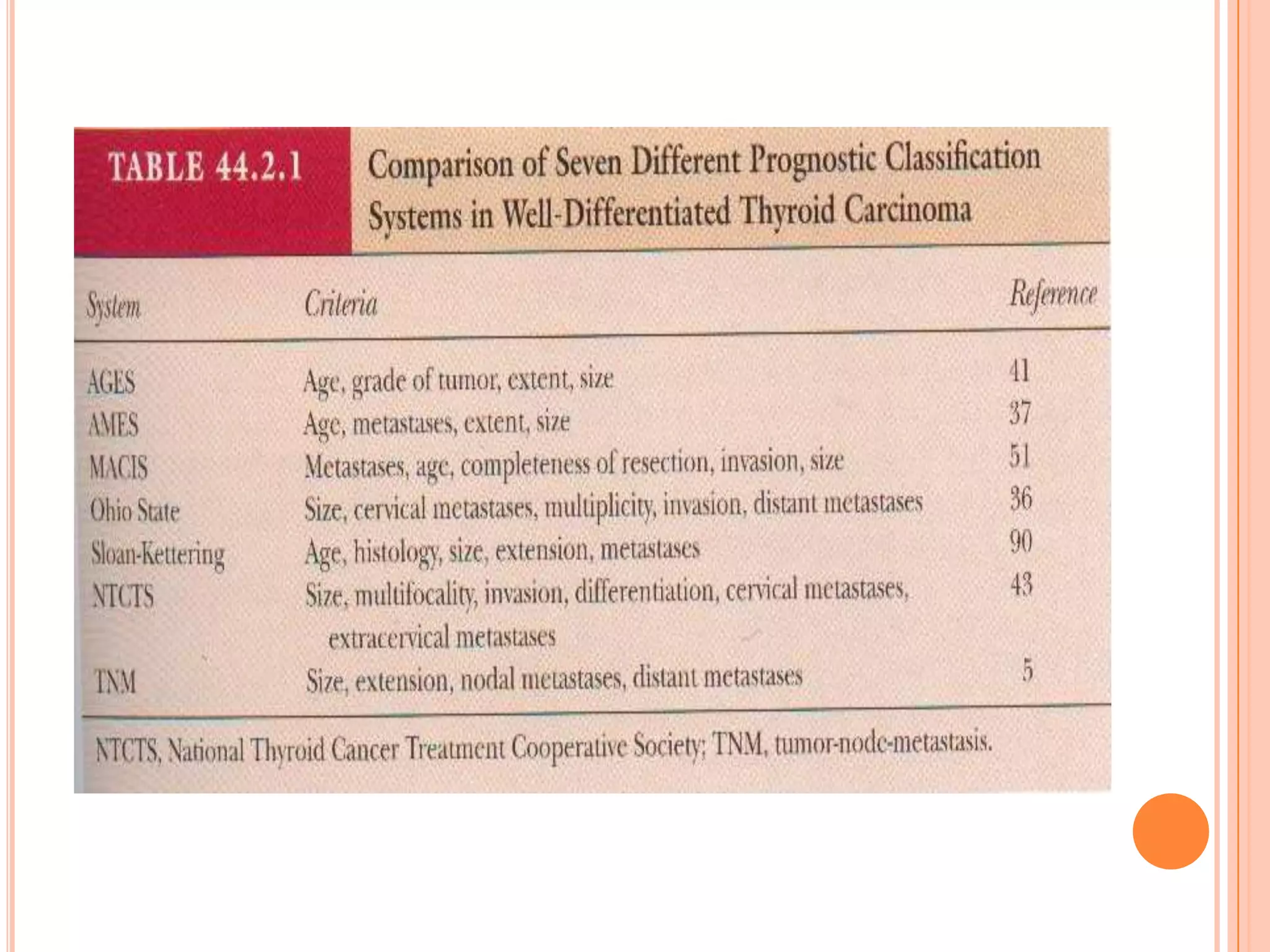
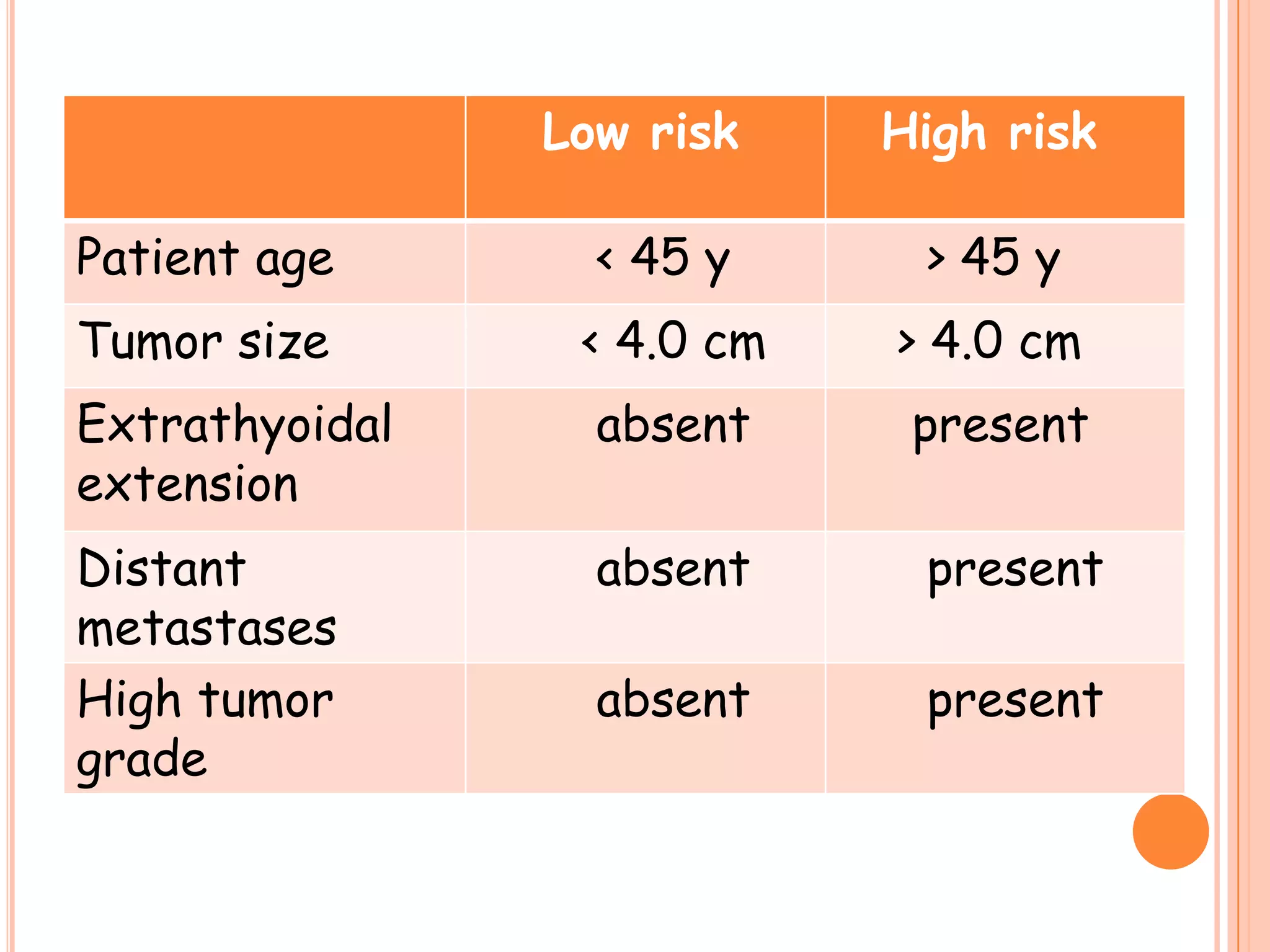

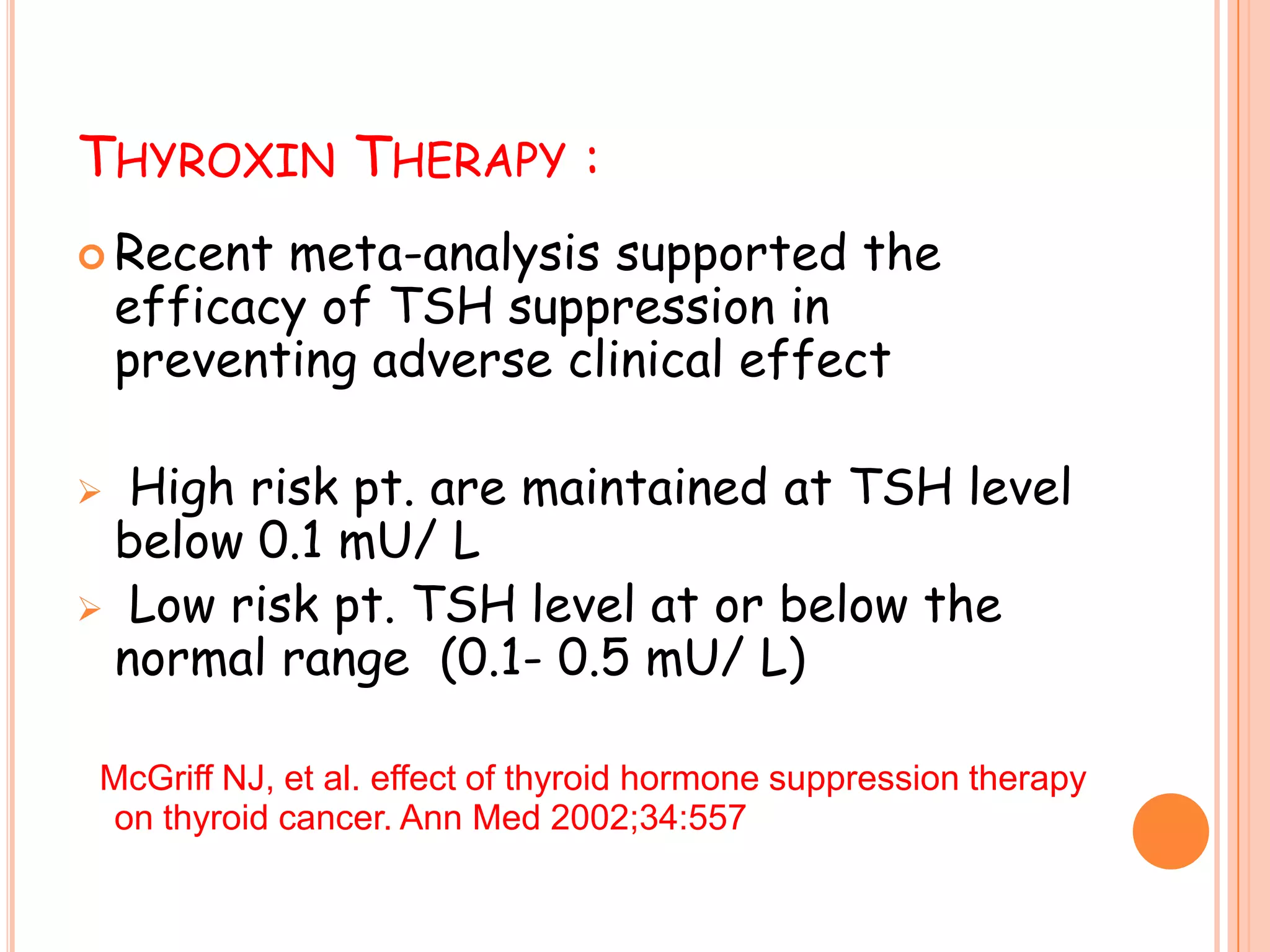
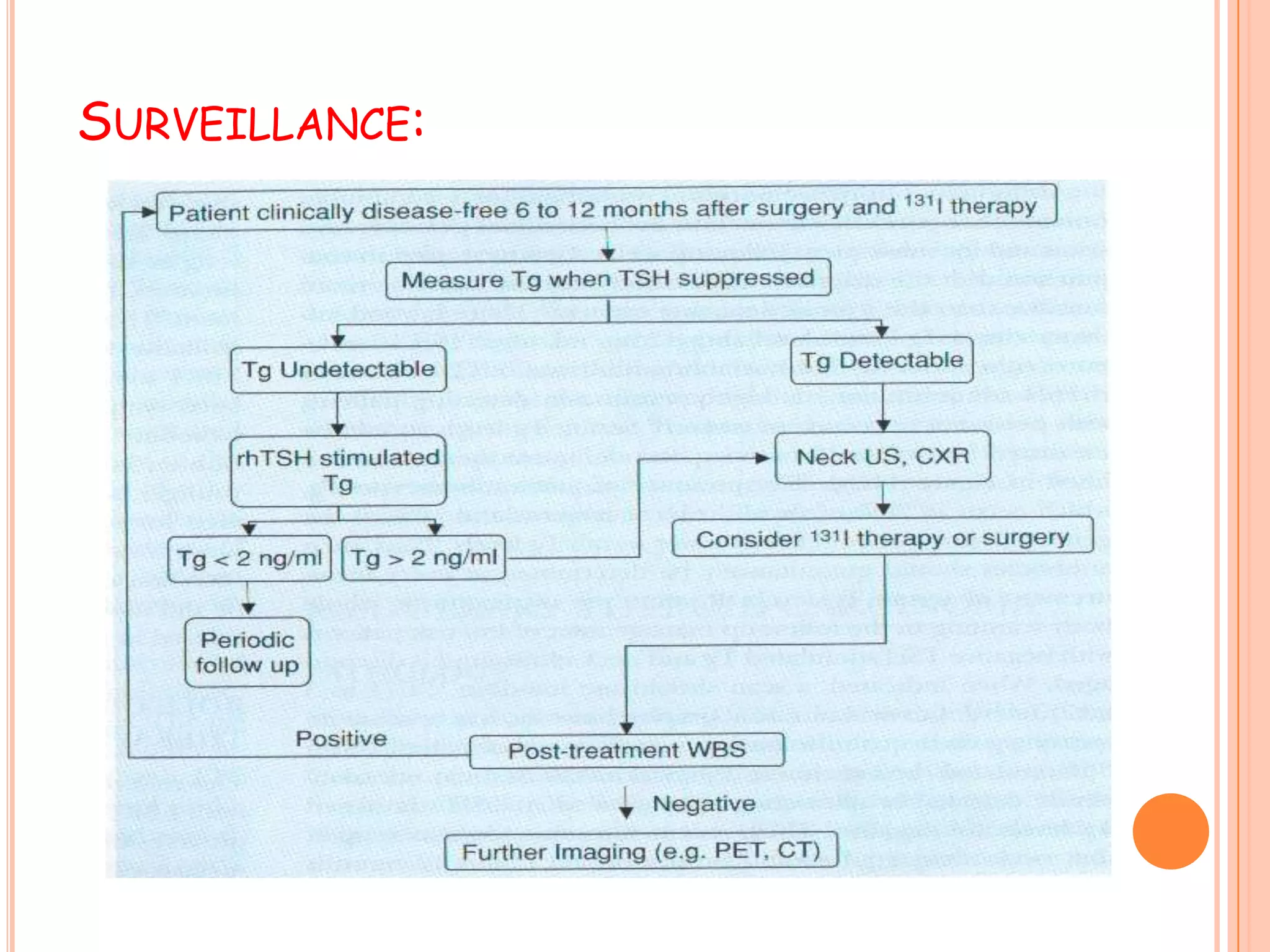
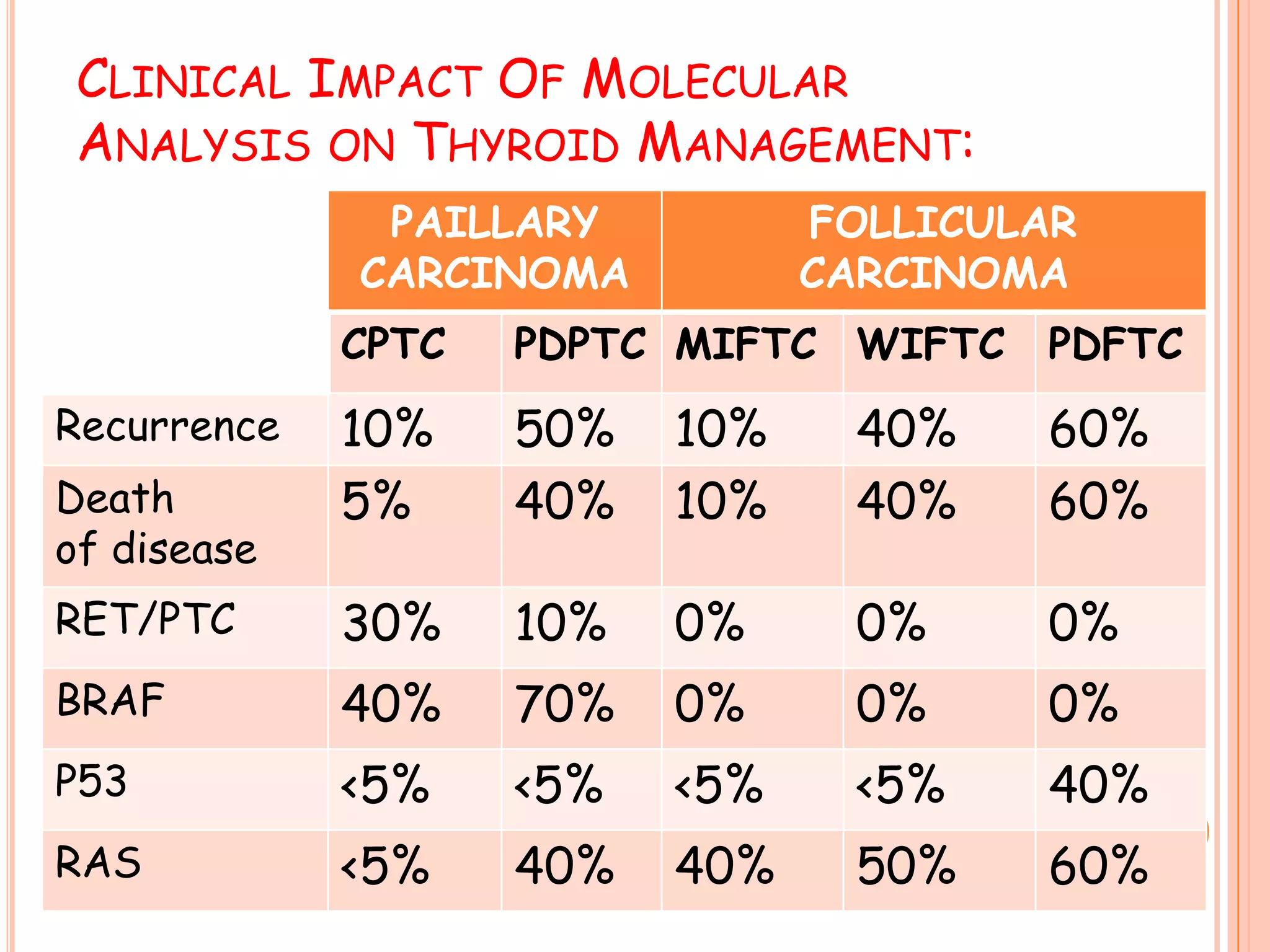




The document discusses various types of thyroid tumors including cancer. It describes the normal anatomy and microscopic picture of the thyroid gland. The primary types of thyroid cancer are papillary, follicular, medullary, and anaplastic originating from the follicular epithelium or parafollicular cells. Risk factors include radiation exposure, family history, iodine deficiency, and thyroiditis. Evaluation involves history, examination, FNAC, ultrasound, and radiological investigations. Treatment depends on cancer type and involves surgery, radioactive iodine, and thyroxine therapy. Prognosis depends on age, tumor size and spread.




















































![Thyroid carcinoma final [part 2]](https://cdn.slidesharecdn.com/ss_thumbnails/thyroidcarcinomafinalpart2-161126043433-thumbnail.jpg?width=640&height=640&fit=bounds)






















































