Downloaded 977 times



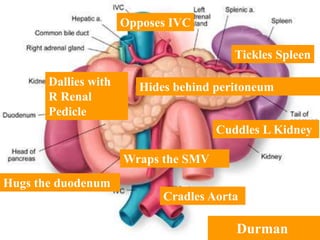

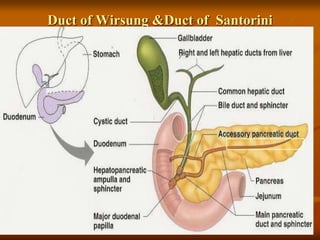
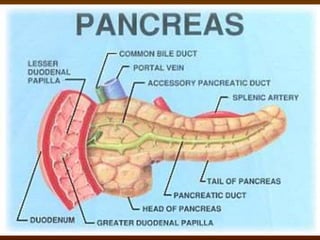












This document outlines a seminar plan on carcinoma of the pancreas presented by Dr. Jyotindra Singh. The seminar will cover topics such as the anatomy and surgical anatomy of the pancreas, pancreatic tumors, modes of presentation, pre-operative workup, various surgeries and surgical videos, recent updates, studies and trials, and a take home message. The seminar introduction discusses that carcinoma of the exocrine pancreas accounts for over 90% of pancreatic tumors and remains an oncologic challenge with a 5-year survival rate of 3%.



















































![Ca pancreas [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/capancreasautosaved-200627065511-thumbnail.jpg?width=640&height=640&fit=bounds)























































