

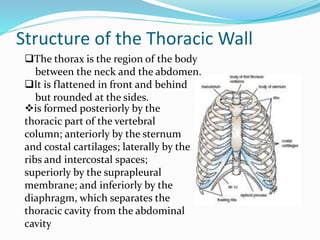
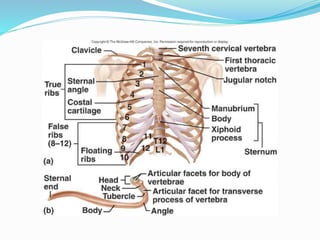

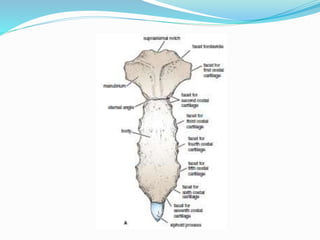
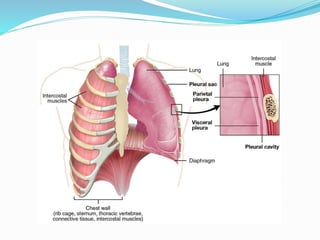
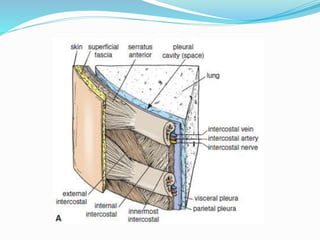


The document provides an overview of the thoracic wall and cavity, detailing its anatomical features including the ribs, sternum, costal cartilages, and diaphragm, as well as their respective functions and relationships. It discusses the thorax's boundaries, divisions, and protective roles, alongside descriptions of various muscular and vascular components within the thoracic region. Additionally, it highlights the importance of the diaphragm in respiration and abdominal pressure management.























































































