
Downloaded 208 times

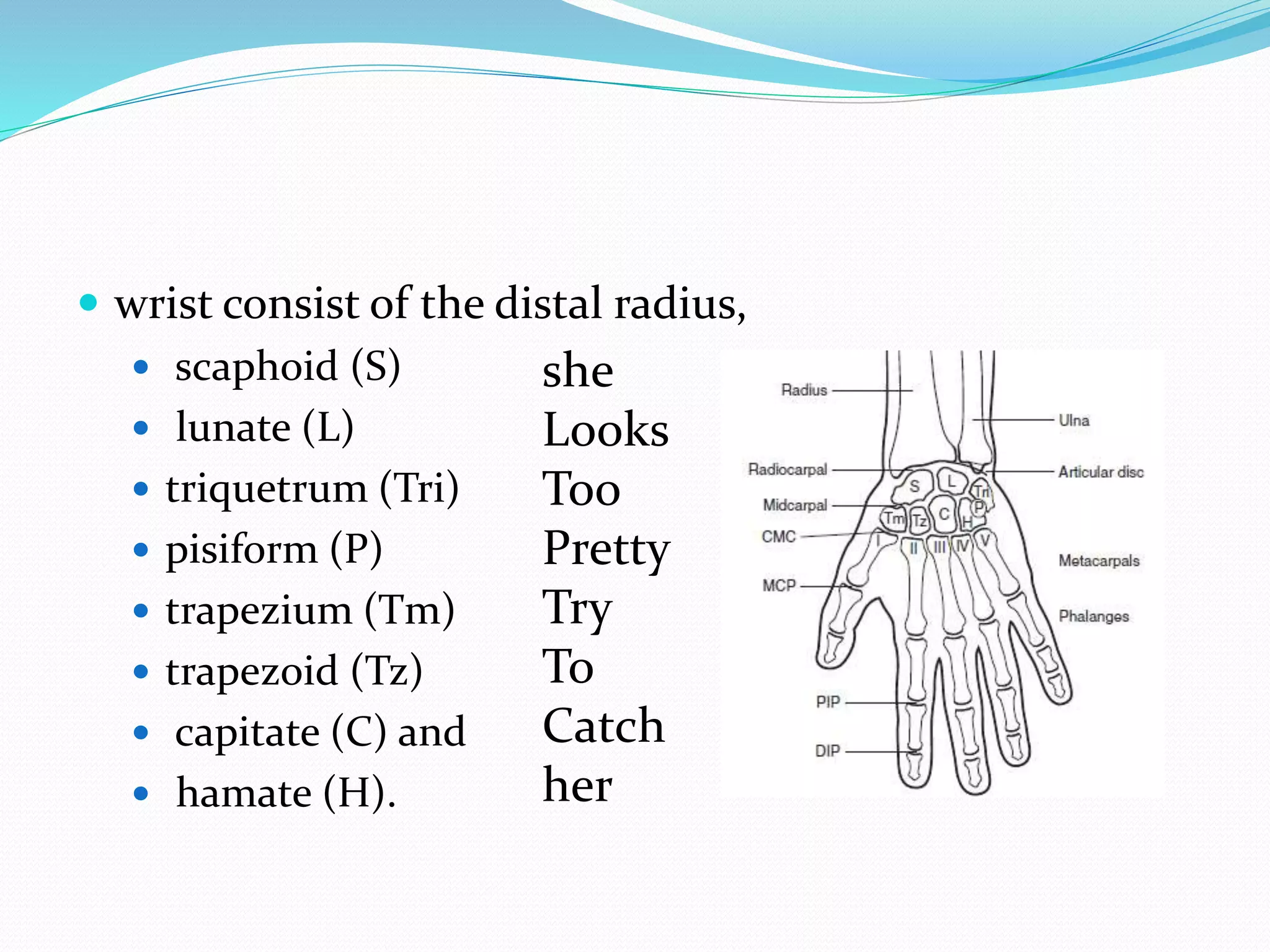
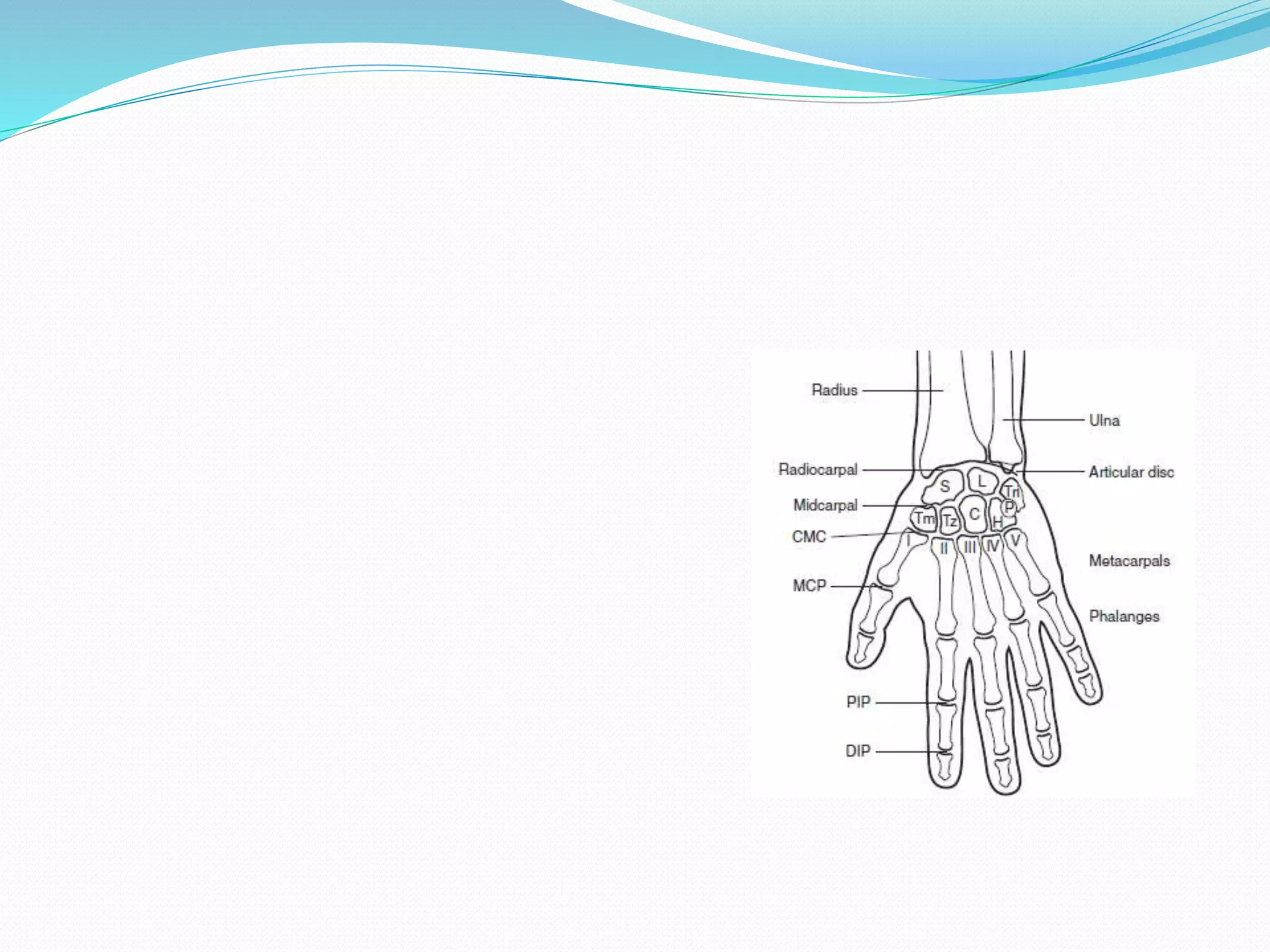





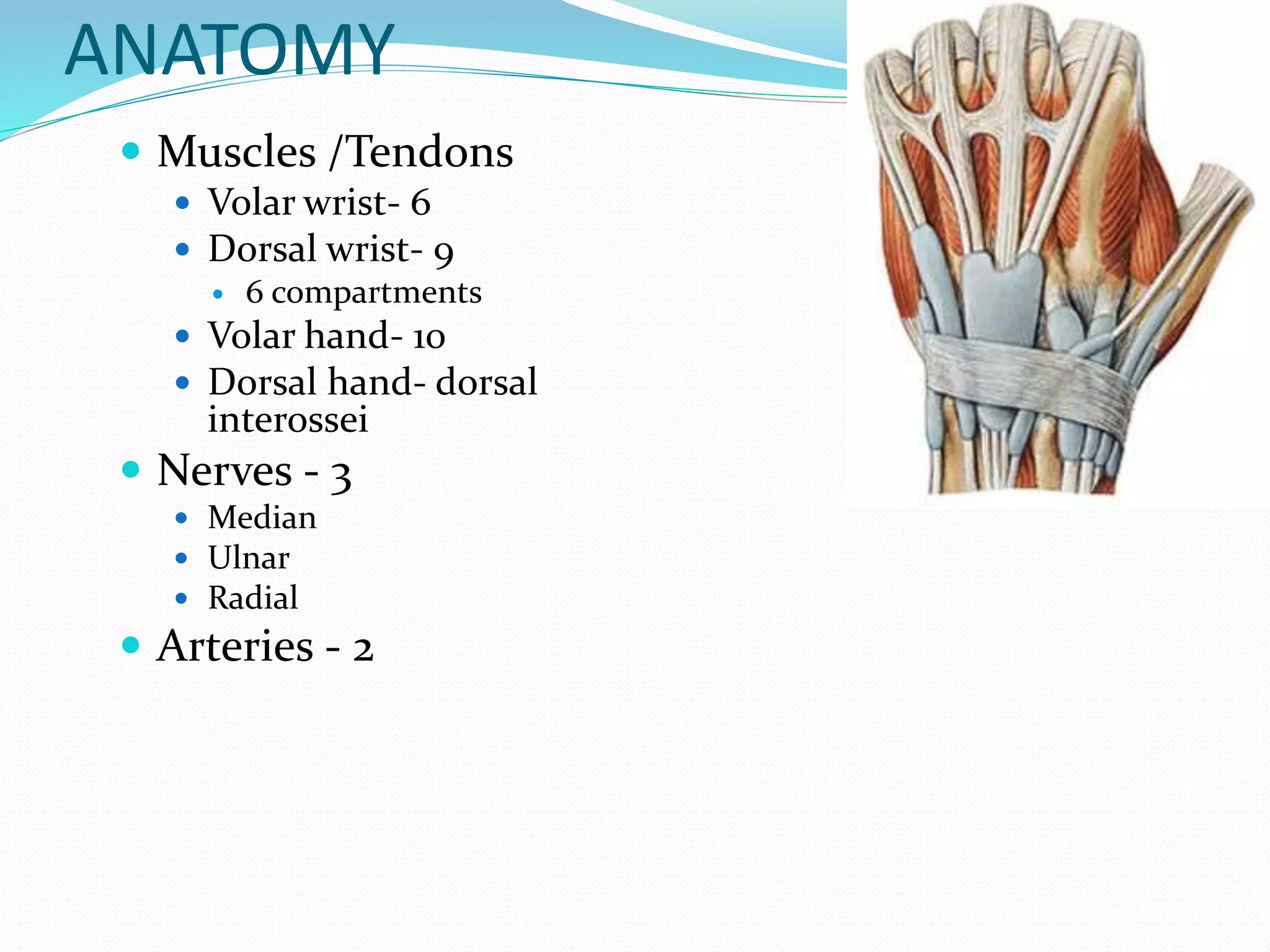



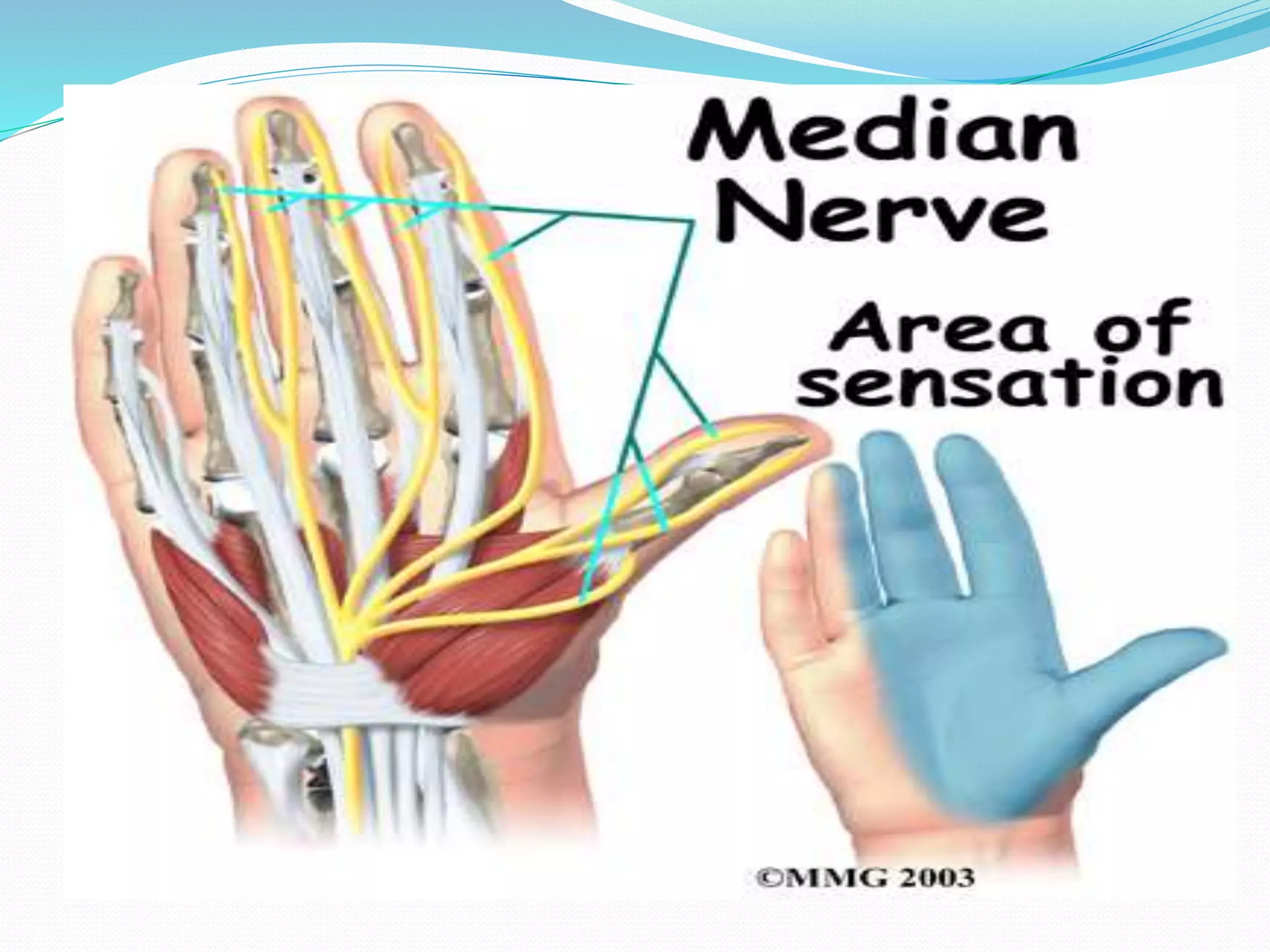


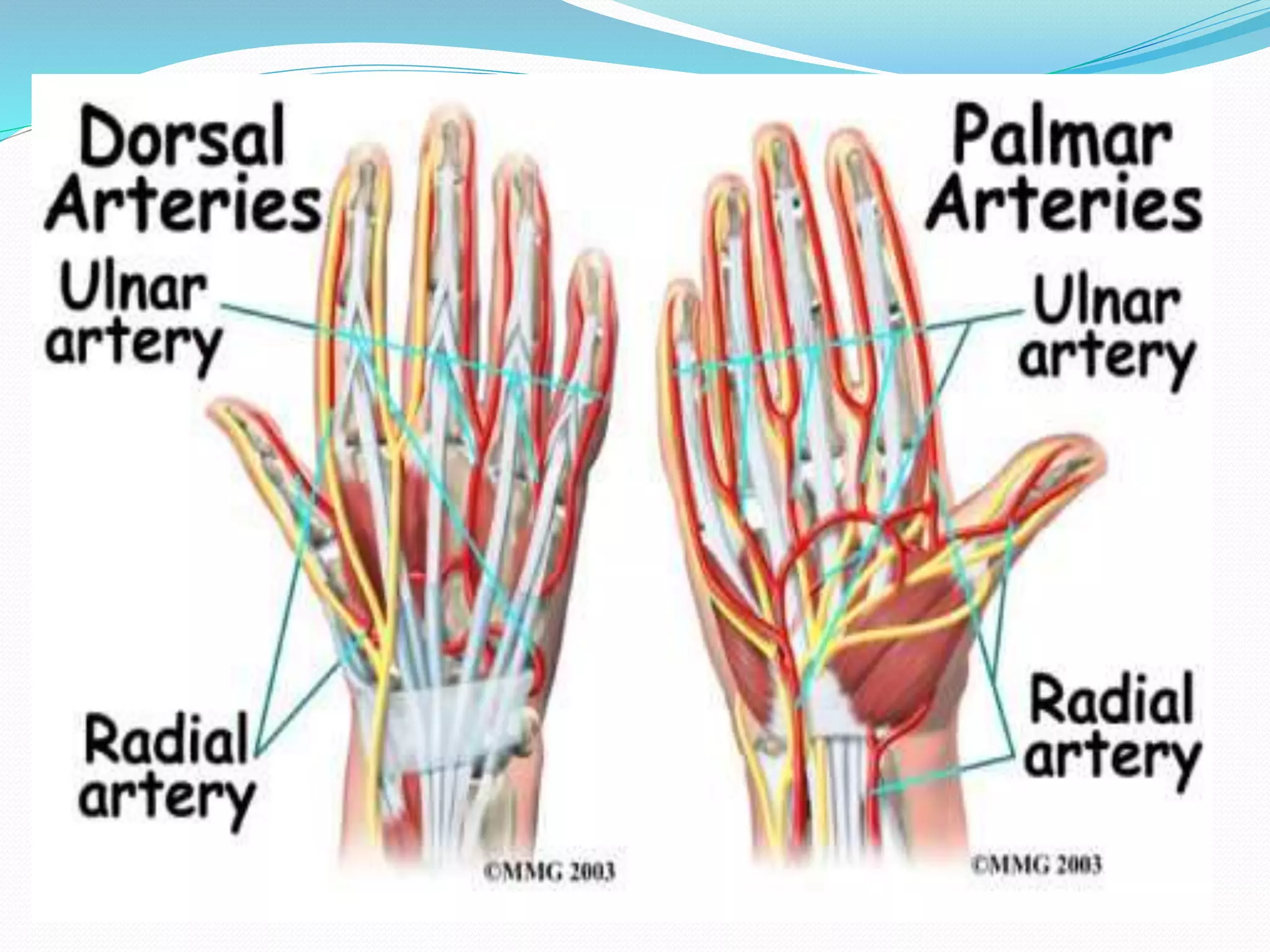

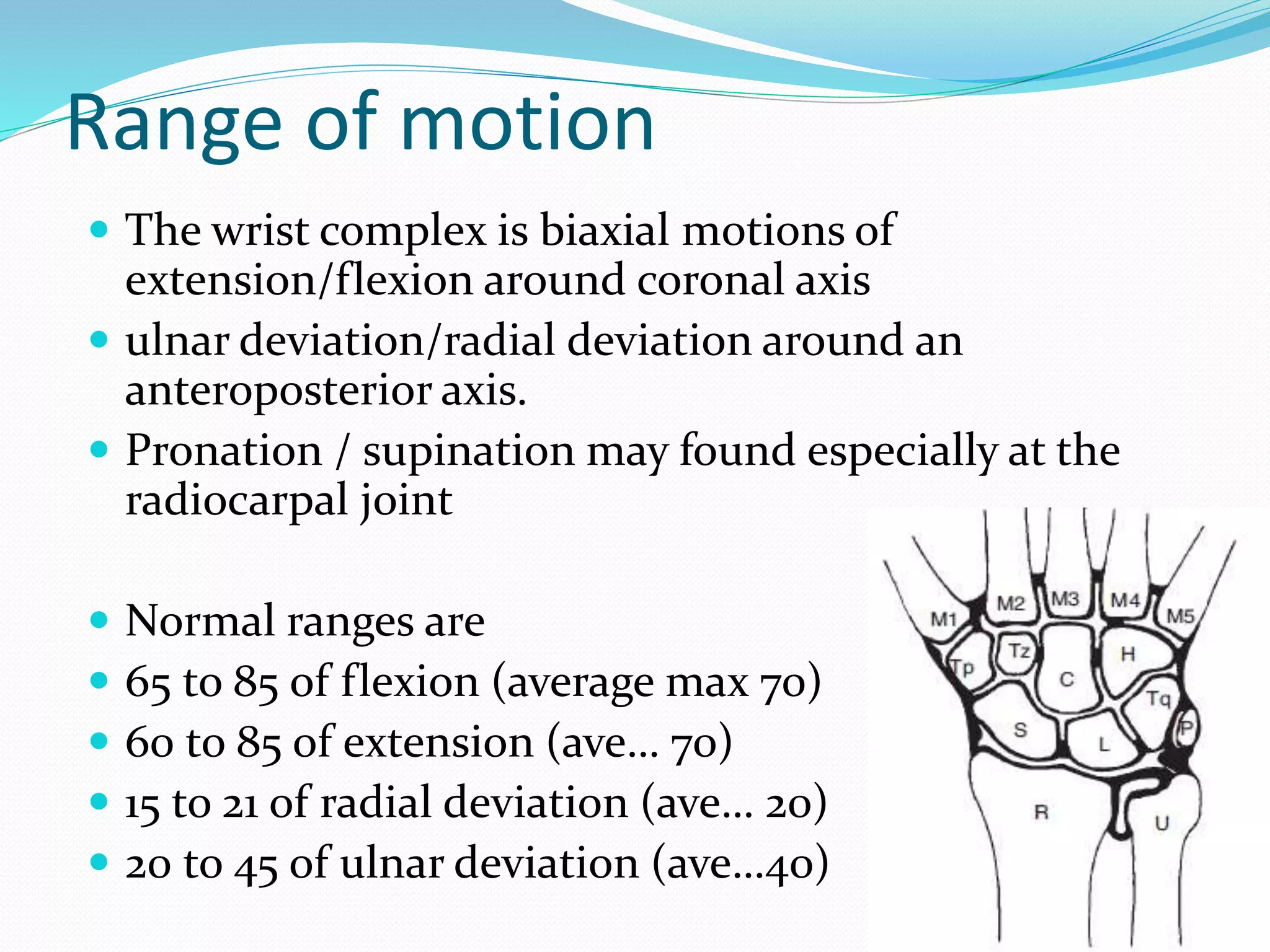


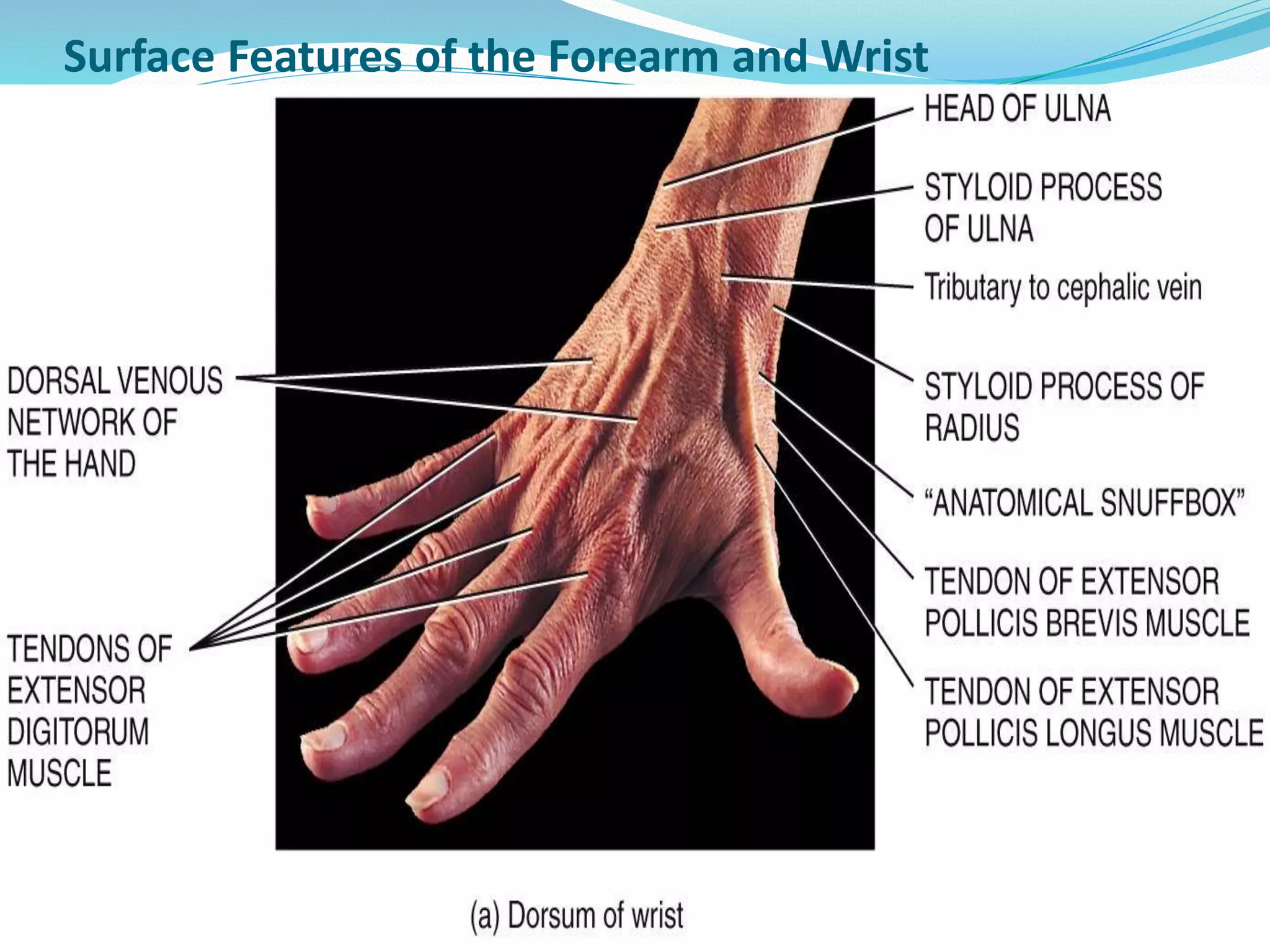

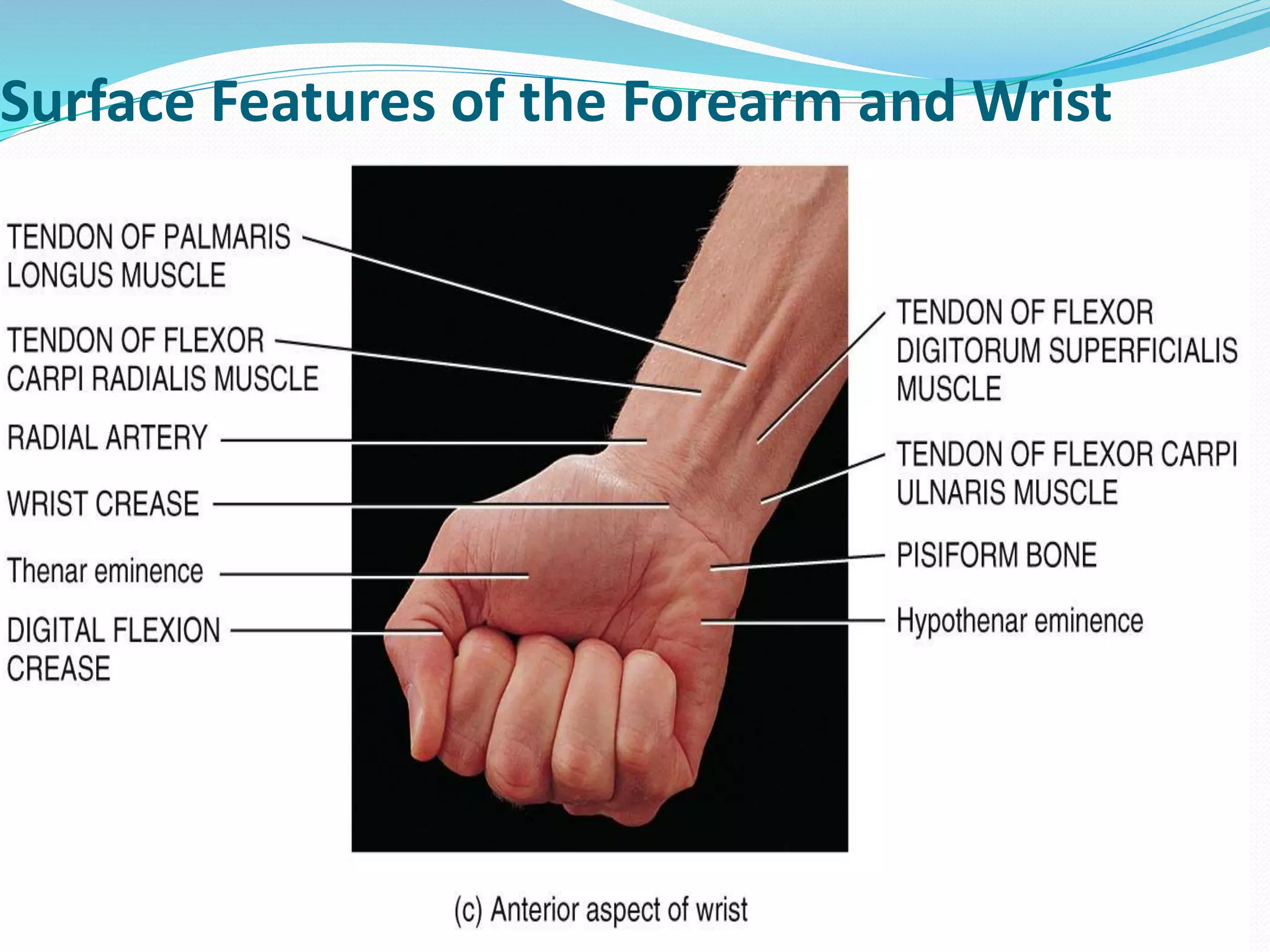

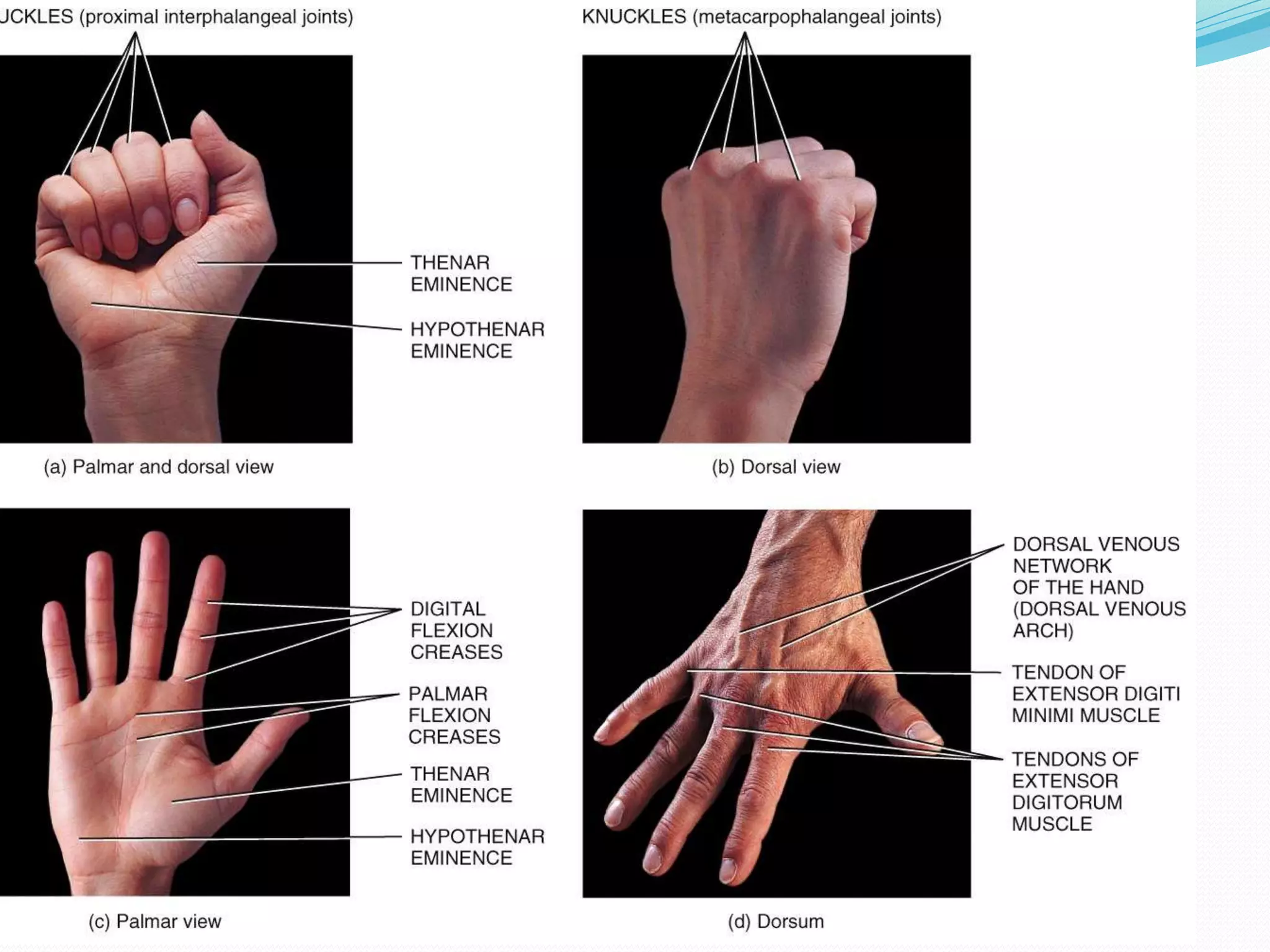
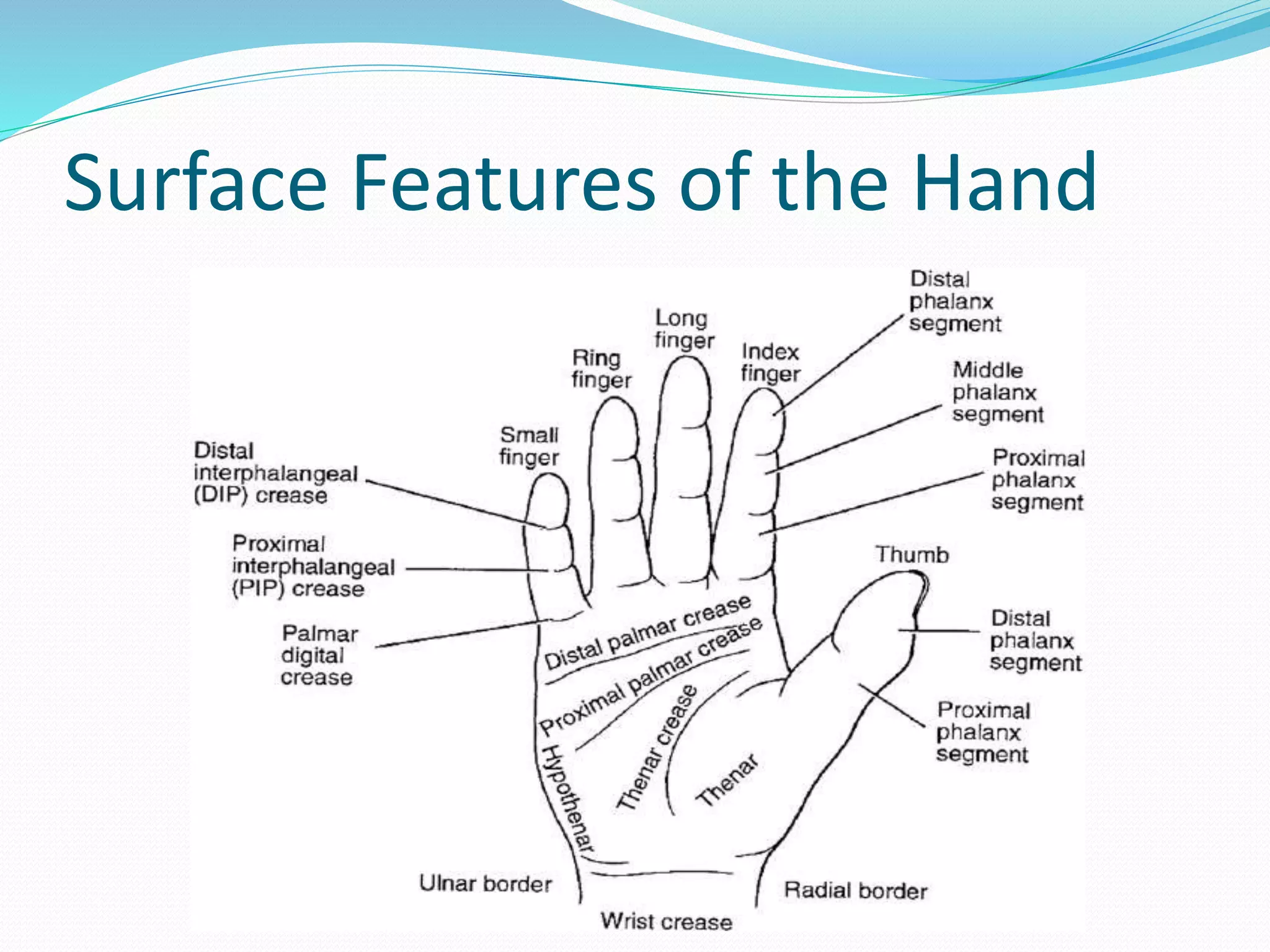



























This document provides information on examining, evaluating, and assessing the hand and wrist. It begins with objectives of reviewing clinical anatomy, performing a physical exam, and discussing common clinical conditions. It then covers anatomy of the bones, joints, muscles, nerves and blood vessels of the wrist and hand. The document provides details on the history, inspection, range of motion assessment, neurologic exam, and special tests like Tinel's sign and Phalen's test used to evaluate common conditions like carpal tunnel syndrome.























































































