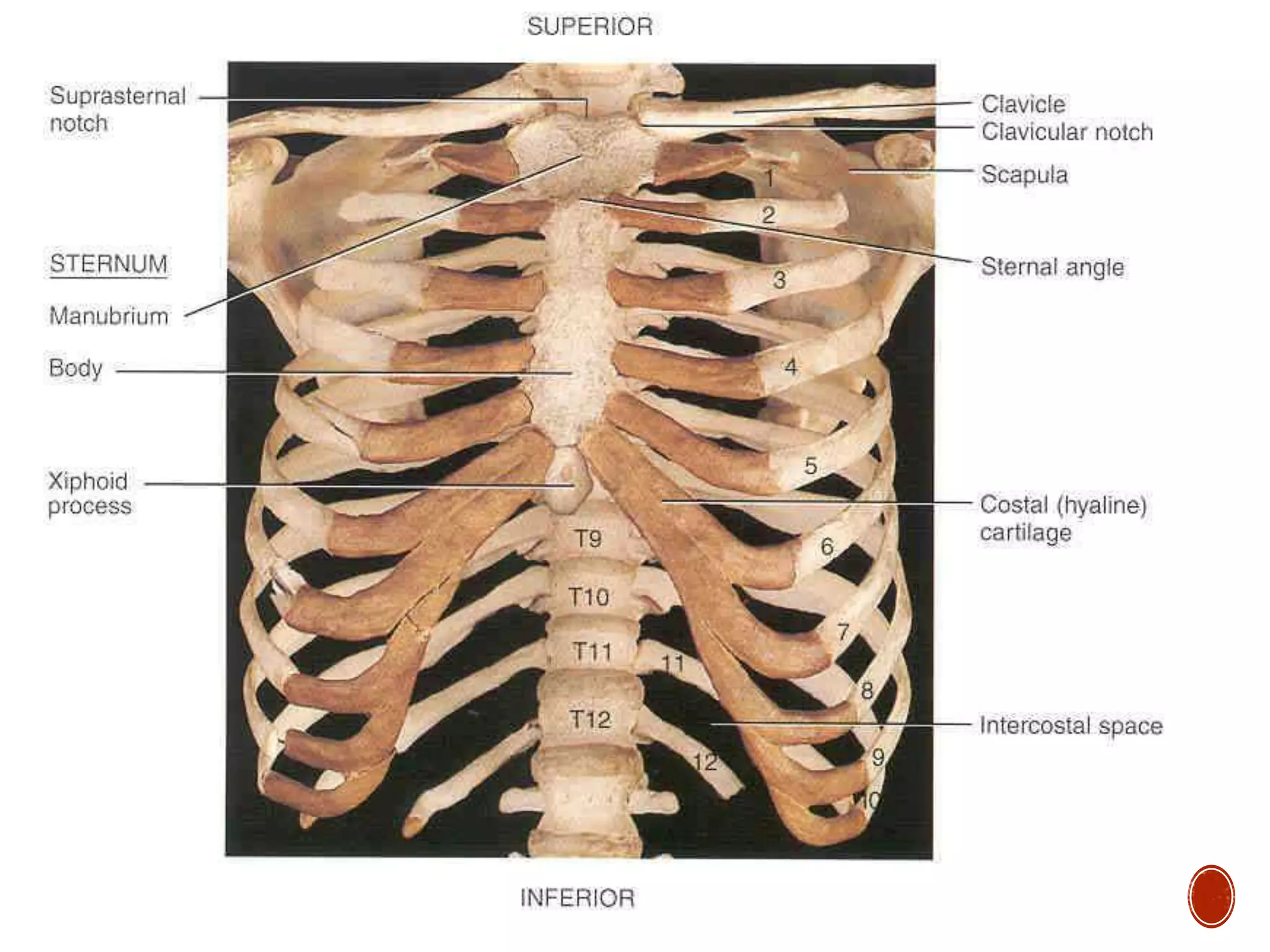
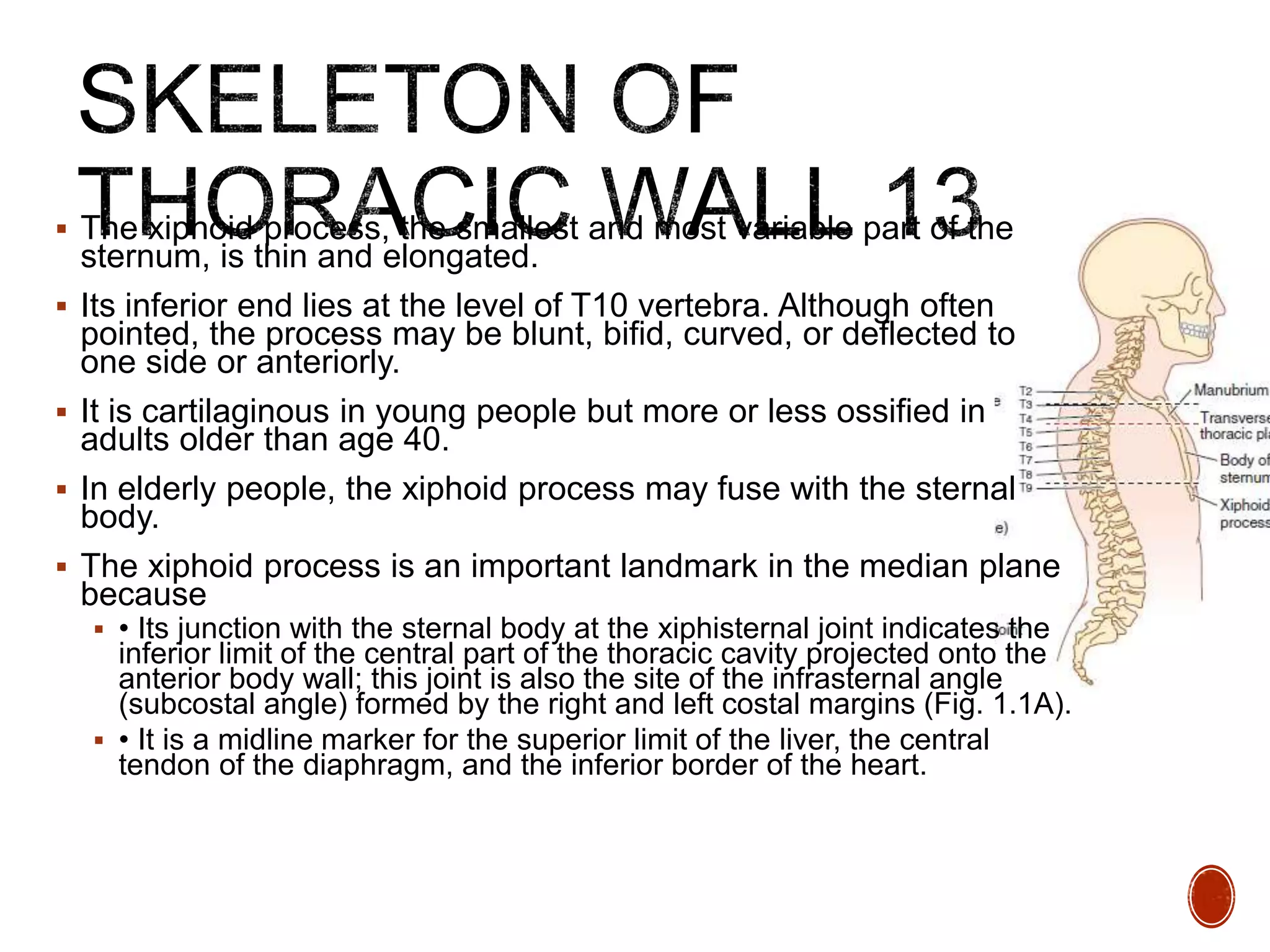
The thoracic cavity contains the heart, lungs, and other structures. It is bounded by the thoracic skeleton which forms a protective cage structure. The thoracic skeleton includes 12 pairs of ribs connected to the sternum anteriorly and thoracic vertebrae posteriorly. The thoracic cavity is divided into the mediastinum and left and right pulmonary cavities housing the lungs. The heart and major blood vessels are also located within the thoracic cavity.