Downloaded 283 times
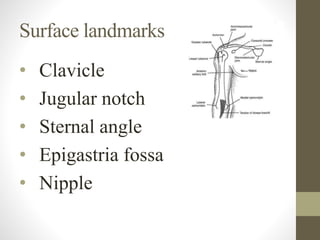
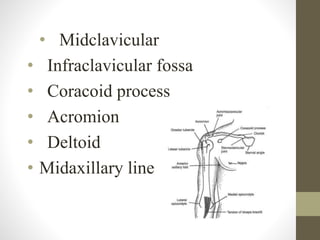
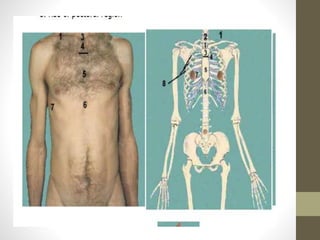
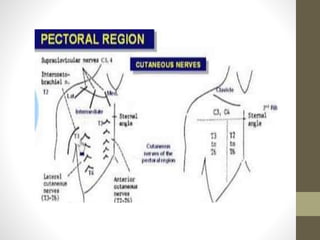
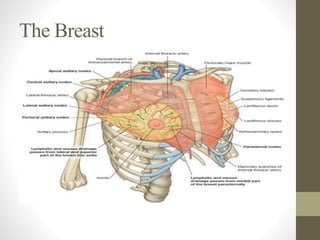
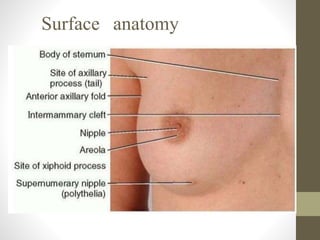
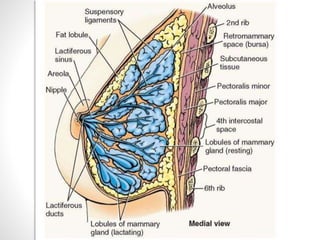
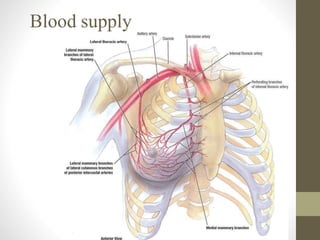
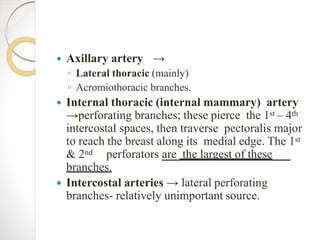
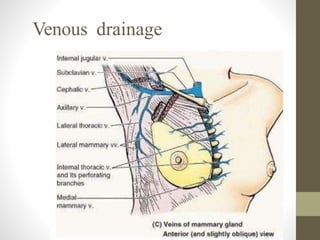
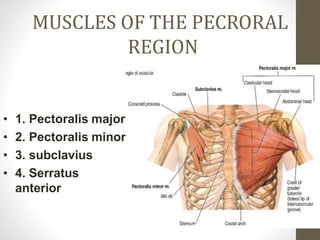
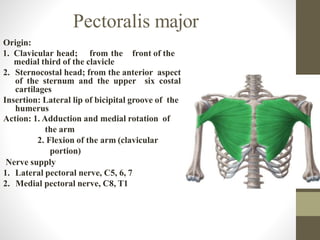

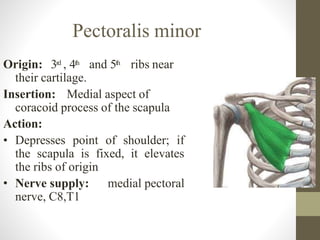
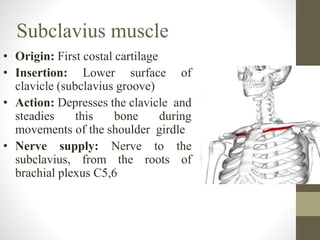
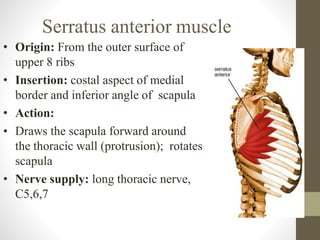
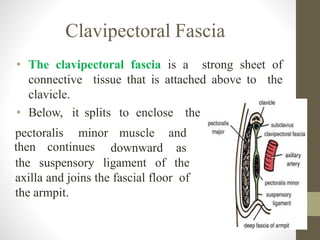


This document provides an overview of the anatomy of the pectoral region. It describes the surface landmarks, superficial fascia containing cutaneous nerves, vessels and the platysma muscle. The breast composition and blood supply are explained. The muscles of the pectoral region including pectoralis major, pectoralis minor, subclavius, and serratus anterior are also detailed. Finally, the clavipectoral fascia enclosing the pectoralis minor is briefly outlined.























































































