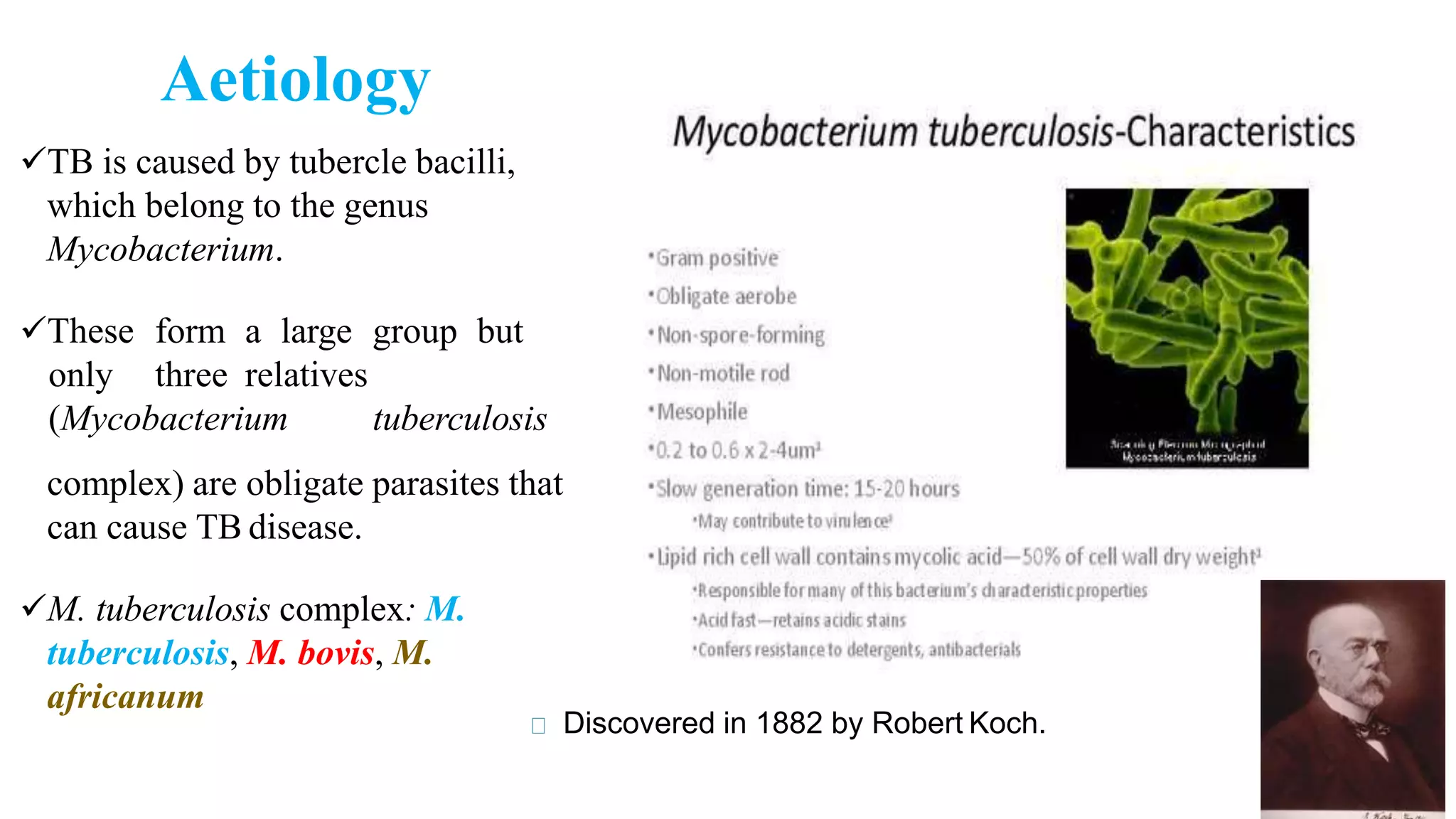
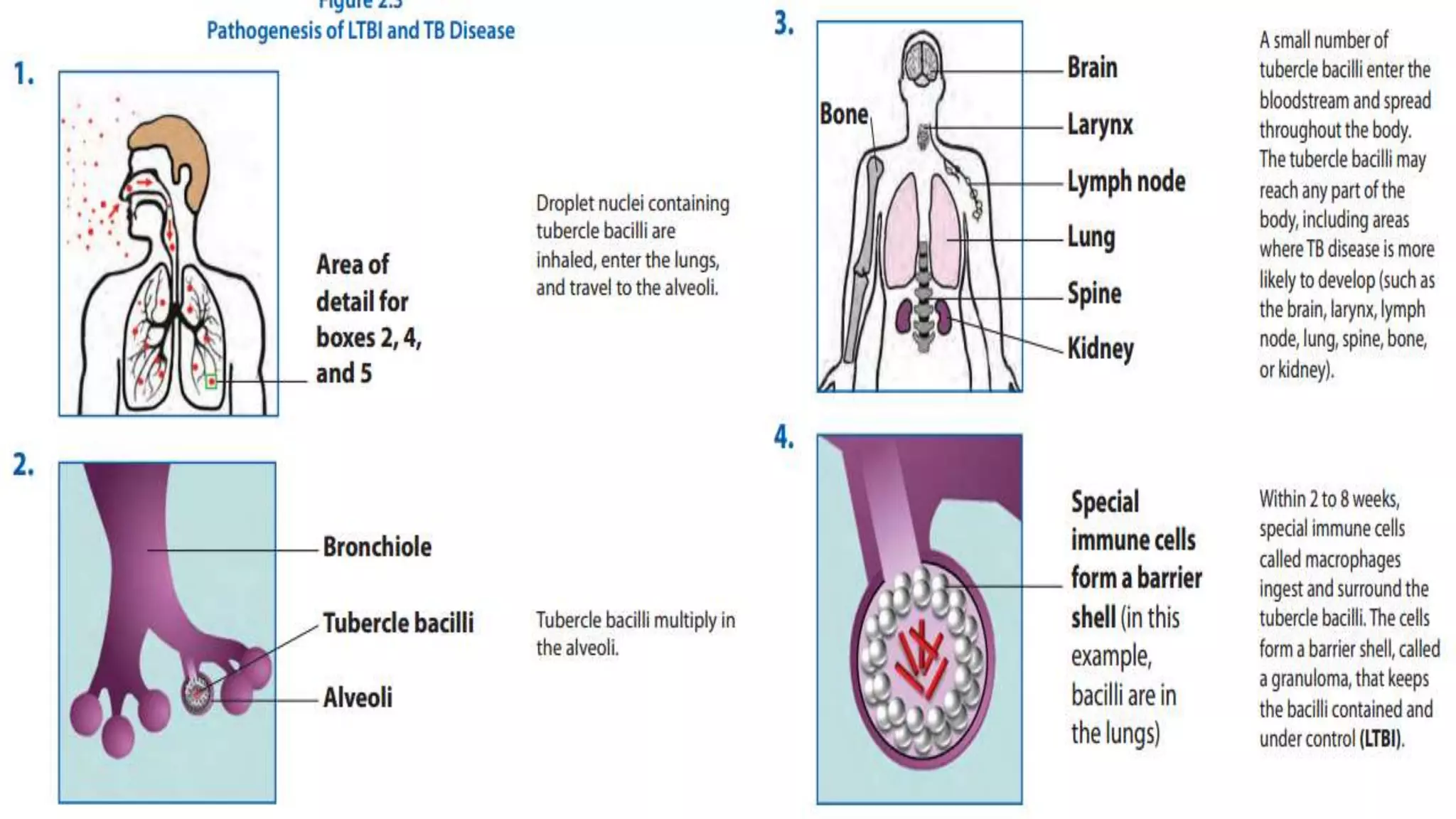
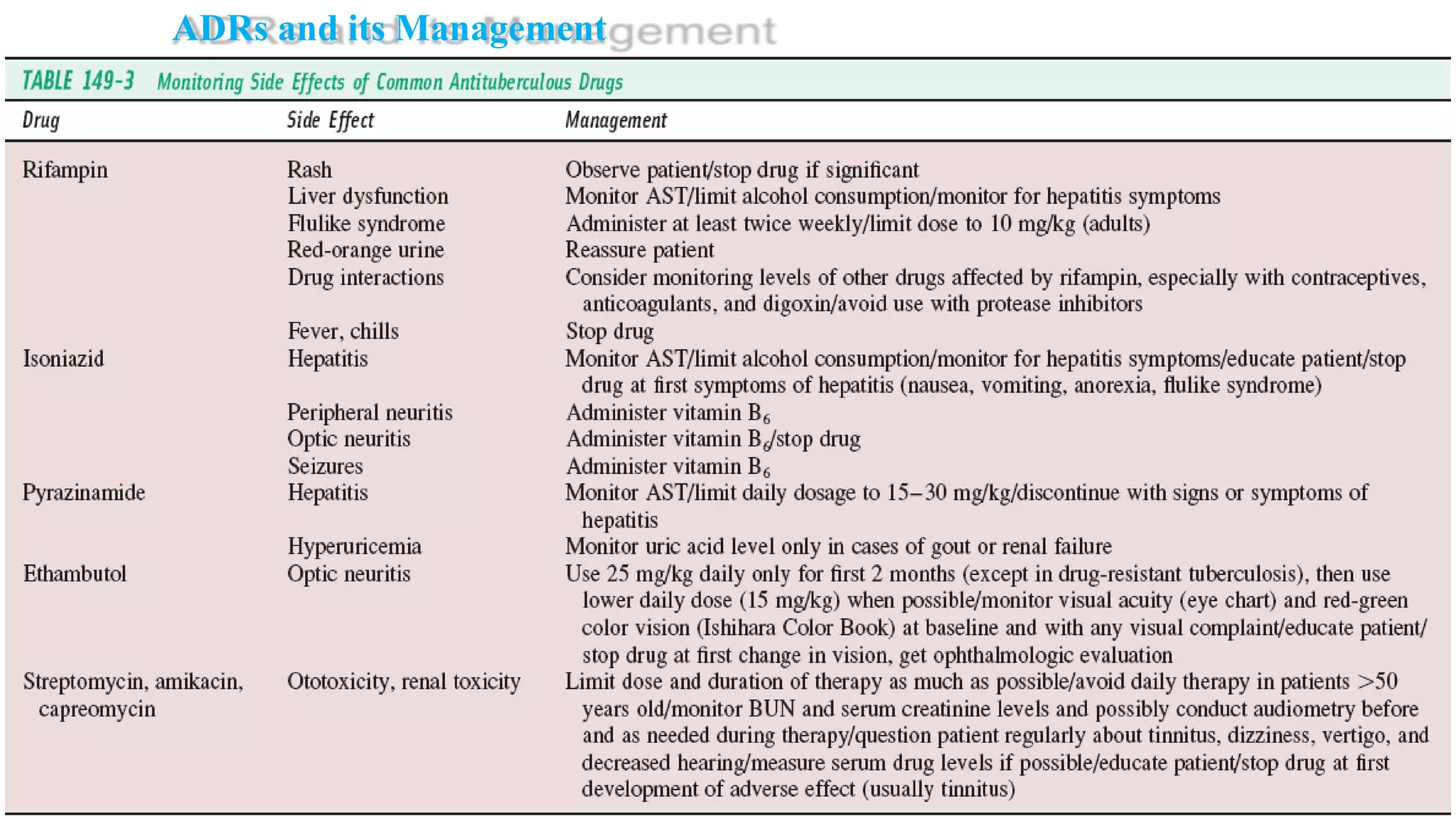
Tuberculosis (TB) is caused by the bacterium Mycobacterium tuberculosis. It typically affects the lungs and can cause symptoms like cough, fever, weight loss, and night sweats. Risk factors include HIV/AIDS, drug use, and other conditions that weaken the immune system. Diagnosis involves tests of sputum, chest x-rays, and tuberculin skin tests. Treatment requires multiple antibiotic drugs taken for 6-9 months. Drug-resistant TB requires specialized treatment with second-line drugs.






































































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)





