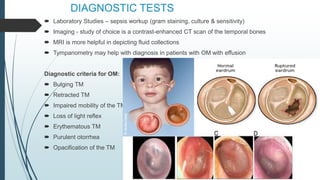
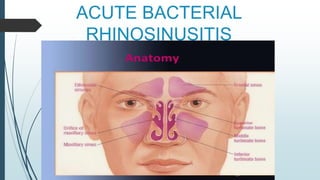
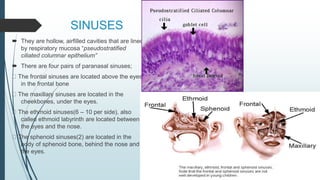
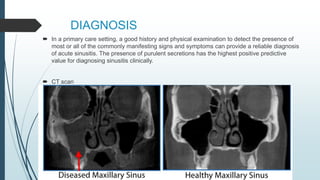
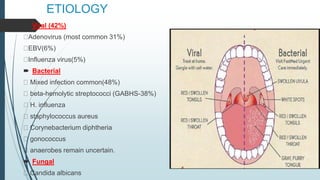
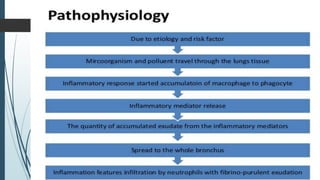
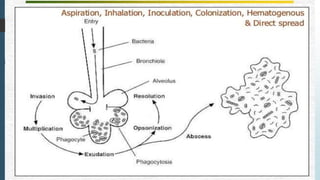
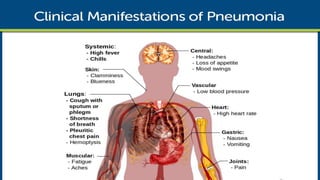
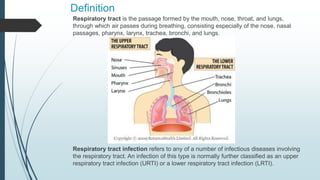
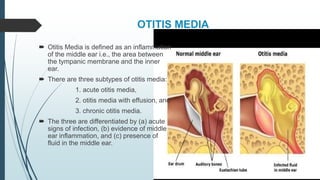
This document discusses respiratory tract infections, specifically focusing on infections of the upper respiratory tract. It defines otitis media as an inflammation of the middle ear and describes its three subtypes. Otitis media is common, especially in young children, and can be caused by bacteria like Streptococcus pneumoniae that enter the middle ear following a viral upper respiratory infection. Symptoms include ear pain, fever, and hearing loss. The document also discusses acute bacterial rhinosinusitis, noting that it is commonly caused by the same bacteria as otitis media and that differentiating between viral and bacterial infections is important to avoid overprescribing antibiotics.

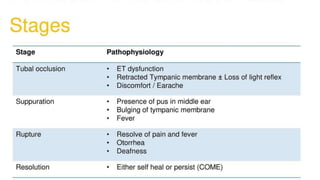
![Stages
1. Catarrhal stage: is characterized by occlusion of
Eustachian tube and congestion of middle ear.
2. Stage of exudation: Exudate collects in the middle ear
and ear drum is pushed laterally. Initially the exudate
is mucoid, later it becomes purulent.
3. Stage of suppuration: Pus in the middle ear collects
under tension, stretches the drum & perforates it by
pressure necrosis & the exudate starts escaping into
external auditory canal
4. Stage of healing: The infection starts resolving from
any of the stages mentioned & usually clears up
completely without leaving any sequelae.
5. Stage of complications: Infection may spread to the
mastoid antrum. Initially it causes Catarrhal mastoiditis
[congestion of the mastoid mucosa], stage of
Coalescent mastoiditis & later empyema of the
mastoid.](https://image.slidesharecdn.com/rti-180914092916/85/Respiratory-tract-infections-Upper-and-Lower-10-320.jpg)