Downloaded 229 times












![OCULAR :
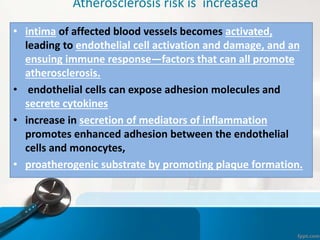
• Amaurosis fugax
• Hypertensive retinopathy [keith-wagner]
arteriolar narrowing, av crossing changes
silver wiring, exudates, papilloedema.
• Ischemic retinopathy [ Uyama and Asayama]
Stage 1 : dilatation of small vessels
stage 2 : micro aneurysm formation
stage 3 : wreath like AV anastamosis
formation surrounding optic
papillae
stage 4 : cataract ,secondary glacoma ,rubeosis,
neo vascularisation, proliferative
retinopathy, vitreous hemorrhage.](https://image.slidesharecdn.com/takayasuarteritis-180722054553/85/Takayasu-arteritis-23-320.jpg)





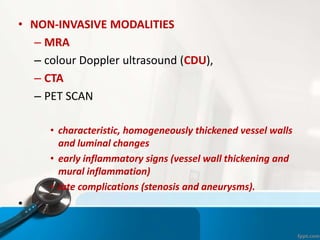





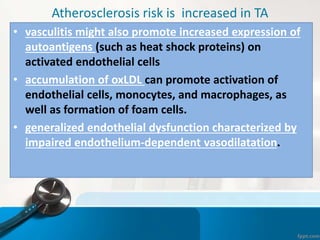




![Steroids in pediatric TA(CMC Vellore)
• Relapse in 15 children at a median duration of 16.5 (9.5- 47 months)
55
Steroids with 2nd line agents 34 (85%)
Remission 30/ 34
Sustained remission till last follow up 15/ 34
Persistent active disease 4
Goel R, Kumar TS, Danda D, Joseph G, Bacon P, Jayaseelan V [unpublished data]
Higher disease progression was observed in patients with persistent active/ relapsing disease](https://image.slidesharecdn.com/takayasuarteritis-180722054553/85/Takayasu-arteritis-49-320.jpg)



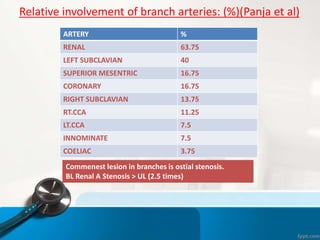
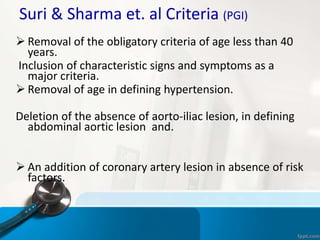
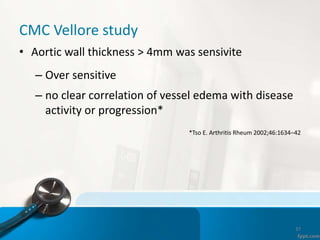
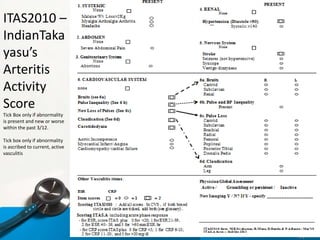
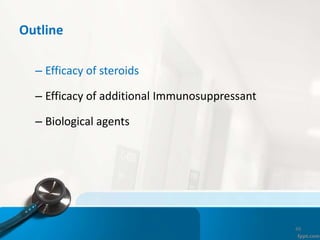
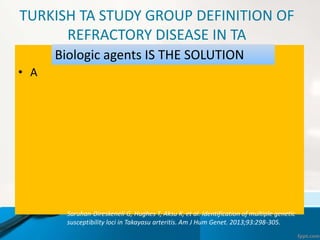
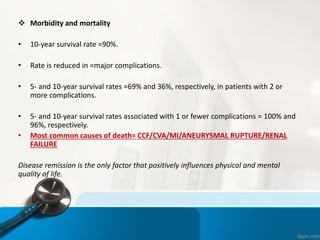
![Mycophenolate & Azathioprine probably better than
Methotrexate (Indirect evidence)
60
0
10
20
30
40
50
60
70
80
90
100
Mtx/Aza/ MMf
used
sustained
remission
improvement
43
28
23
100 100
19
50
15
96
methotrexate based*
azathioprine based ** (n= 15/65) at 1yr
follow up
mycophenolate based$ (n=19/40)
Adult TA (MMf)% (n=21/21)
No.ofpatients(%)
Maksimowicz-Mc Kinnon etal. A& R 2007; 56 (3); 1000-1009
Valsakumar AK etal. J Rheumatol. 2003;30(8):1793-8
Goel R, Kumar TS, Danda D, Joseph G, Jayaseelan V. [unpublished]
Goel R, Danda D, Mathew J, Edwin N. Clin Rheumatol (2010) 29:329–332](https://image.slidesharecdn.com/takayasuarteritis-180722054553/85/Takayasu-arteritis-54-320.jpg)











- Takayasu Arteritis is an idiopathic inflammatory disease that causes inflammation and narrowing of the large arteries, mainly the aorta and its branches. - Early diagnosis is difficult due to nonspecific initial symptoms. Management is challenging due to the lack of reliable disease activity markers and low levels of evidence regarding treatment. - High-dose corticosteroids are effective for inducing remission but relapses often occur upon tapering. Additional immunosuppressants are usually needed to sustain remission and prevent disease progression and damage.












































![Takayasu_Arteritis_-_A_review_(1)[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/takayasuarteritis-areview11-240416070529-93b99a9c-thumbnail.jpg?width=640&height=640&fit=bounds)










































