Downloaded 266 times

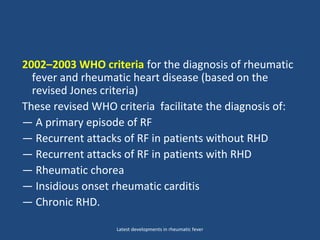


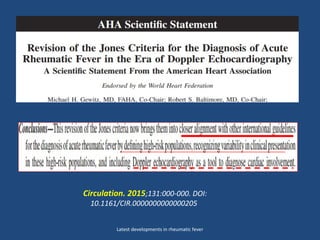
![(Modified from Parry E, Godfrey R, Mabey D, Gill G [eds]:
Principles of Medicine in Africa. 3rd ed. Cambridge, Cambridge
University Press, 2004, p 861.)
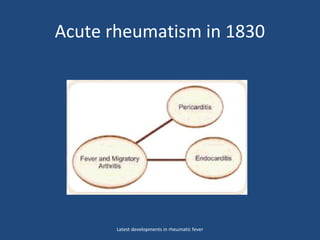
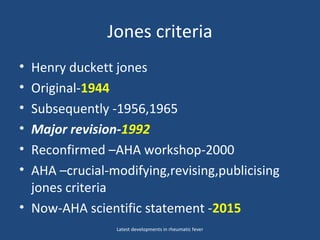
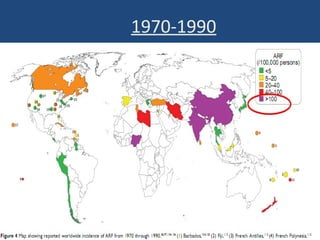
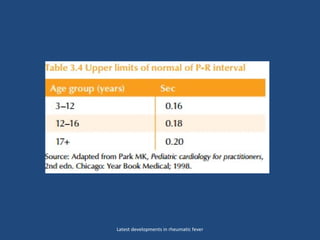
• 4 patterns RF in 150 years.
–
A- Preantibiotic fall in the incidence of
ARF of industrialized countries
– B-Persistent high incidence RF
[Africa and south Asia].
– C-Postantibiotic fall in the incidence
of rheumatic fever in countries that
instituted comprehensive programs for
primary and secondary prevention of
rheumatic fever, such as Cuba, Costa
Rica, Martinique, and Guadeloupe.
– D-Fall and rise in the incidence of
rheumatic fever in the formerly Soviet
Republics of Central Asia.
Latest developments in rheumatic fever](https://image.slidesharecdn.com/latestdevelopmentsindiagnosisofrheumaticfever-180722120456/85/acute-rheumatic-fever-28-320.jpg)
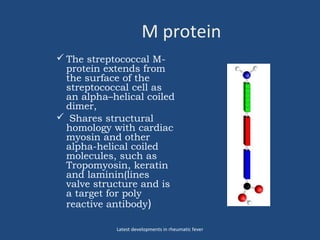
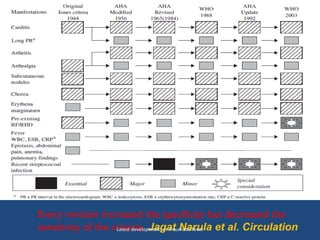
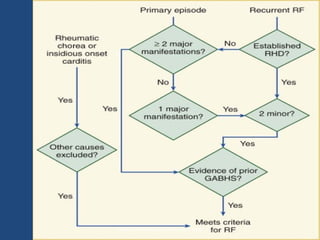
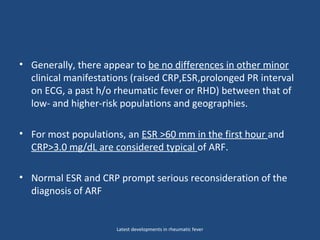
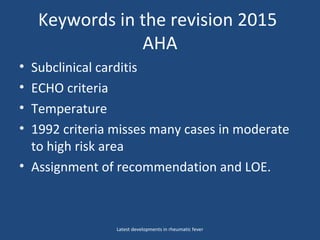
![• Aschoff nodule of acute
rheumatic fever. The nodule is
composed of Anitschkow cells;
these have clear nuclei with a
central bar of chromatin, said to
resemble a caterpillar. There is a
central area of fibrin. This central
necrosis is further surrounded by
a mononuclear cell infiltrate.
Myocardial fibres adjacent to the
Aschoff body are undergoing
Fibrinoid necrosis. (Sebire NJ,
Ashworth M, Malone M, Jacques
TS [eds]: Diagnostic Pediatric
Surgical Pathology. Churchill
Livingstone, United Kingdom,
2010.)
Latest developments in rheumatic fever](https://image.slidesharecdn.com/latestdevelopmentsindiagnosisofrheumaticfever-180722120456/85/acute-rheumatic-fever-39-320.jpg)
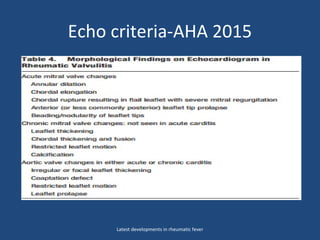
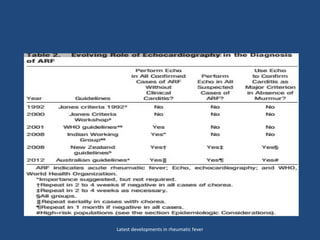
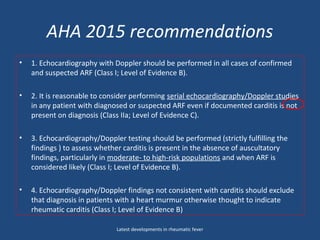




1) The document discusses the history and latest developments in rheumatic fever, including the evolution of diagnostic criteria from Jones in 1944 to the 2015 AHA statement. 2) Key topics covered include subclinical carditis, the role of echocardiography in diagnosis, revisions to arthritis criteria, and implications of epidemiology for diagnostic approaches. 3) The 2015 AHA statement recommends echocardiography for all suspected rheumatic fever cases and considers monoarthritis a possible manifestation in high-risk populations.




























![Acute Rheumatic Fever – An Update[6704].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/acuterheumaticfeveranupdate6704-250603154932-9410381d-thumbnail.jpg?width=640&height=640&fit=bounds)























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


