Downloaded 1,175 times




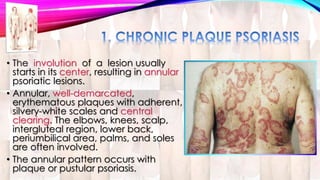
















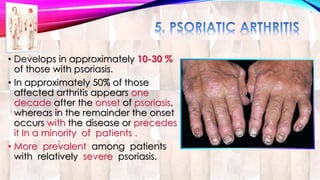
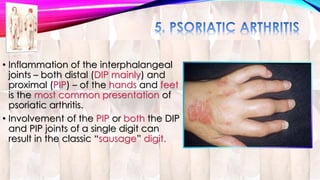


























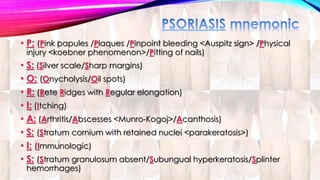







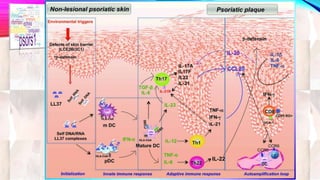

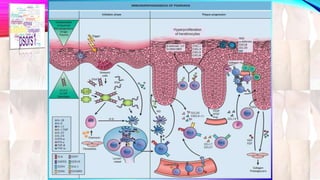



Psoriasis is a chronic immune-mediated disorder with a genetic basis influenced by environmental factors, affecting about 2% of the global population. It presents with characteristic erythematous plaques and has significant impacts on quality of life, with up to 30% of patients developing psoriatic arthritis. The condition can manifest in various forms and severity, with symptoms including itching, localized redness, and scaling, and can be exacerbated by stress or environmental factors.
















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)














