Downloaded 22 times
![Types and CausesTypes and Causes
of Hypertensionof Hypertension
(Systolic and(Systolic and
Diastolic)Diastolic)
Essential Hypertension (90% to 95% of Cases)Essential Hypertension (90% to 95% of Cases)
Secondary HypertensionSecondary Hypertension
RENALRENAL
Acute glomerulonephritisAcute glomerulonephritis
Chronic renal diseaseChronic renal disease
Polycystic diseasePolycystic disease
Renal artery stenosisRenal artery stenosis
Renal vasculitisRenal vasculitis
Renin-producing tumorsRenin-producing tumors
ENDOCRINEENDOCRINE
Adrenocortical hyperfunction (Cushing syndrome, primary Adrenocortical hyperfunction (Cushing syndrome, primary
aldosteronism, congenital adrenal hyperplasia, licorice aldosteronism, congenital adrenal hyperplasia, licorice
ingestion)ingestion)
Exogenous hormones (glucocorticoids, estrogen [including Exogenous hormones (glucocorticoids, estrogen [including
pregnancy-induced and oral contraceptives], pregnancy-induced and oral contraceptives],
sympathomimetics and tyramine-containing foods, sympathomimetics and tyramine-containing foods,
monoamine oxidase inhibitors)monoamine oxidase inhibitors)
PheochromocytomaPheochromocytoma
AcromegalyAcromegaly
Hypothyroidism (myxedema)Hypothyroidism (myxedema)
Hyperthyroidism (thyrotoxicosis)Hyperthyroidism (thyrotoxicosis)
Pregnancy-inducedPregnancy-induced
CARDIOVASCULARCARDIOVASCULAR
Coarctation of aortaCoarctation of aorta
Polyarteritis nodosaPolyarteritis nodosa
Increased intravascular volumeIncreased intravascular volume
Increased cardiac outputIncreased cardiac output
Rigidity of the aortaRigidity of the aorta
NEUROLOGICNEUROLOGIC
PsychogenicPsychogenic
Increased intracranial pressureIncreased intracranial pressure
Sleep apneaSleep apnea
Acute stress, including surgeryAcute stress, including surgery](https://image.slidesharecdn.com/hypertentionppt-181017150303/85/Hypertention-ppt-8-320.jpg)
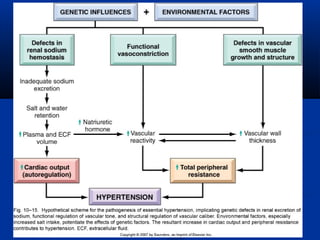

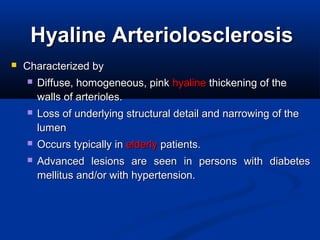
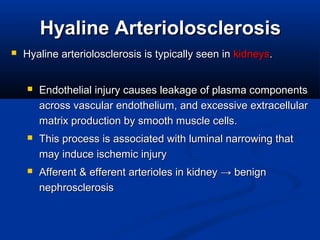
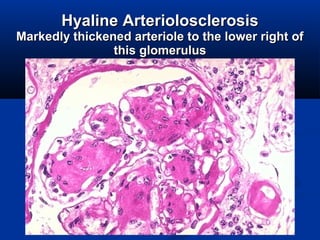
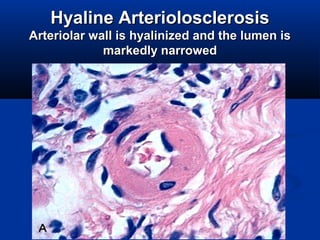
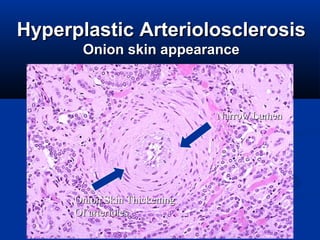
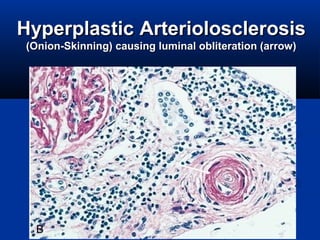
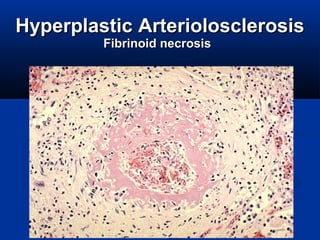

This document discusses hypertension and cardiovascular pathology. It defines hypertension as elevated blood pressure, and notes that systolic blood pressure is more important in determining cardiovascular risk. Hypertension typically remains asymptomatic and contributes to coronary heart disease, strokes, and other conditions. The document discusses essential hypertension as the cause of 90-95% of cases and its genetic and environmental risk factors. It also describes vascular pathology associated with hypertension such as hyaline arteriolosclerosis, which involves thickening of arteriole walls and can induce ischemic injury, particularly in the kidneys.


















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)




