Downloaded 120 times
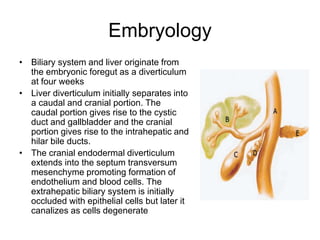
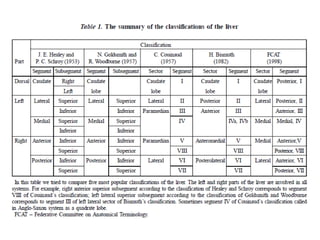
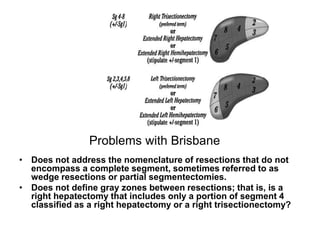
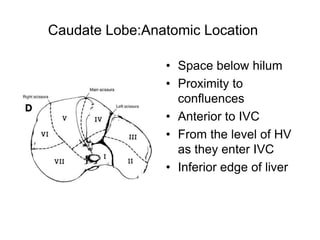
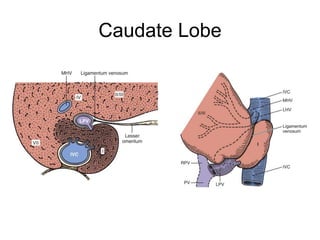
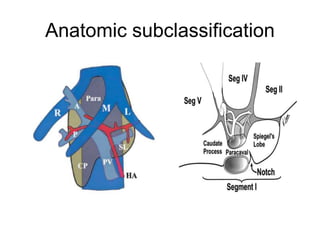


The liver has significant anatomic variability. It develops from the foregut and is divided into lobes based on vascular and biliary anatomy. The caudate lobe is located posteriorly between the IVC and other lobes. It has complex vascular and biliary drainage patterns. The liver is commonly divided into segments based on Couinaud's or Brisbane's classifications to describe resection types. The caudate lobe specifically can be further divided into the Spiegel lobe, caudate process, and paracaval portion.





















































































