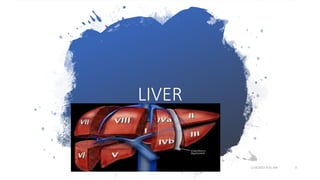
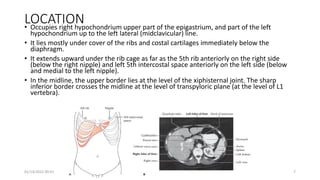
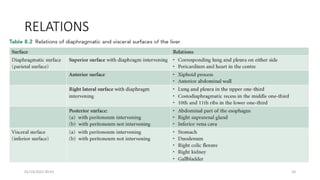
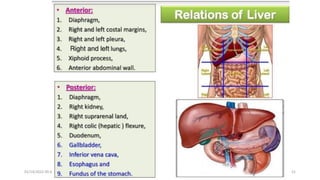
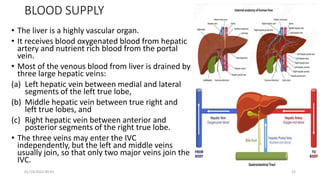
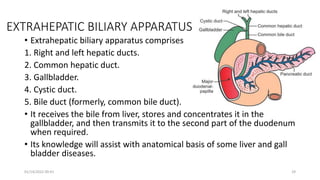
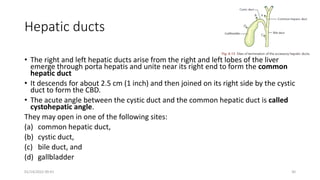
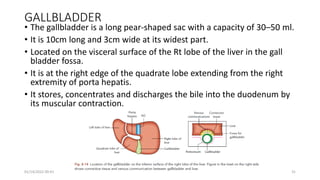
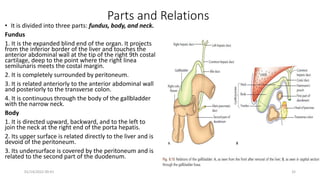
The document provides information about the liver and extrahepatic biliary apparatus. It describes the location, lobes, segments, blood supply, and lymphatic drainage of the liver. It also discusses the porta hepatis and relations of the liver. Additionally, it provides information about the gallbladder, cystic duct, and common bile duct. The objectives are to describe the anatomy and features of the liver and related structures.