The document summarizes CT anatomy of the liver in 3 sentences:
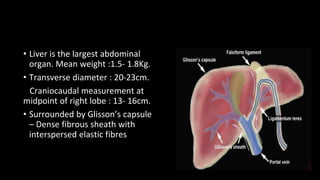
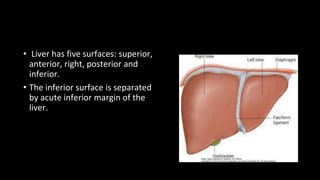
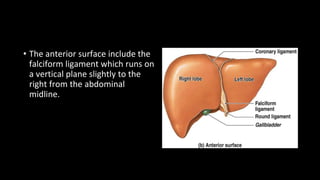
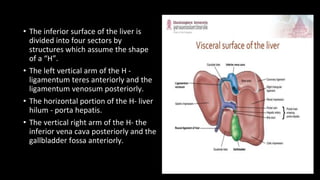
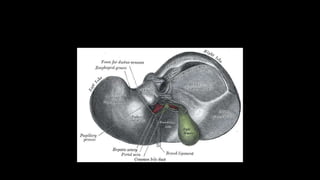
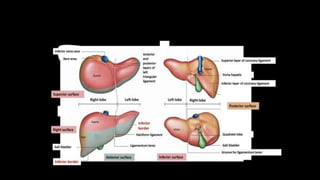
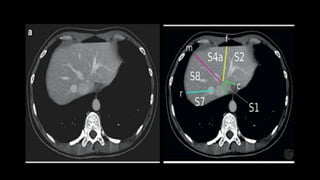
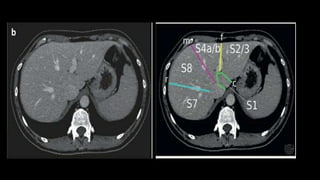
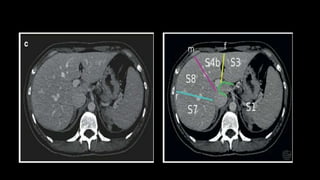
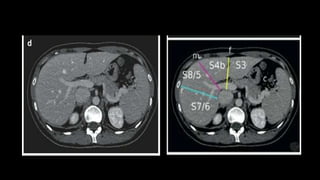
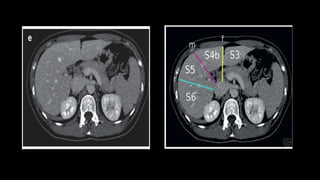
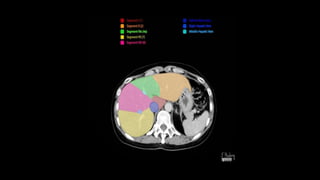
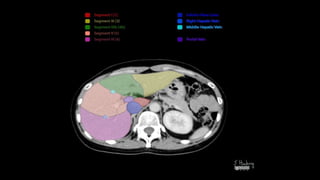
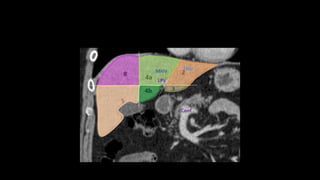
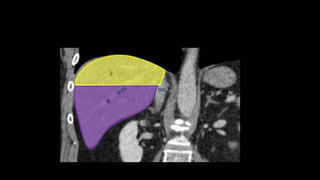
The liver is the largest abdominal organ, surrounded by Glisson's capsule. It has five surfaces and is divided into four sectors by structures forming an "H" on its inferior surface. The liver has eight functionally independent segments based on its vascular inflow, outflow and biliary drainage.