Downloaded 1,689 times
























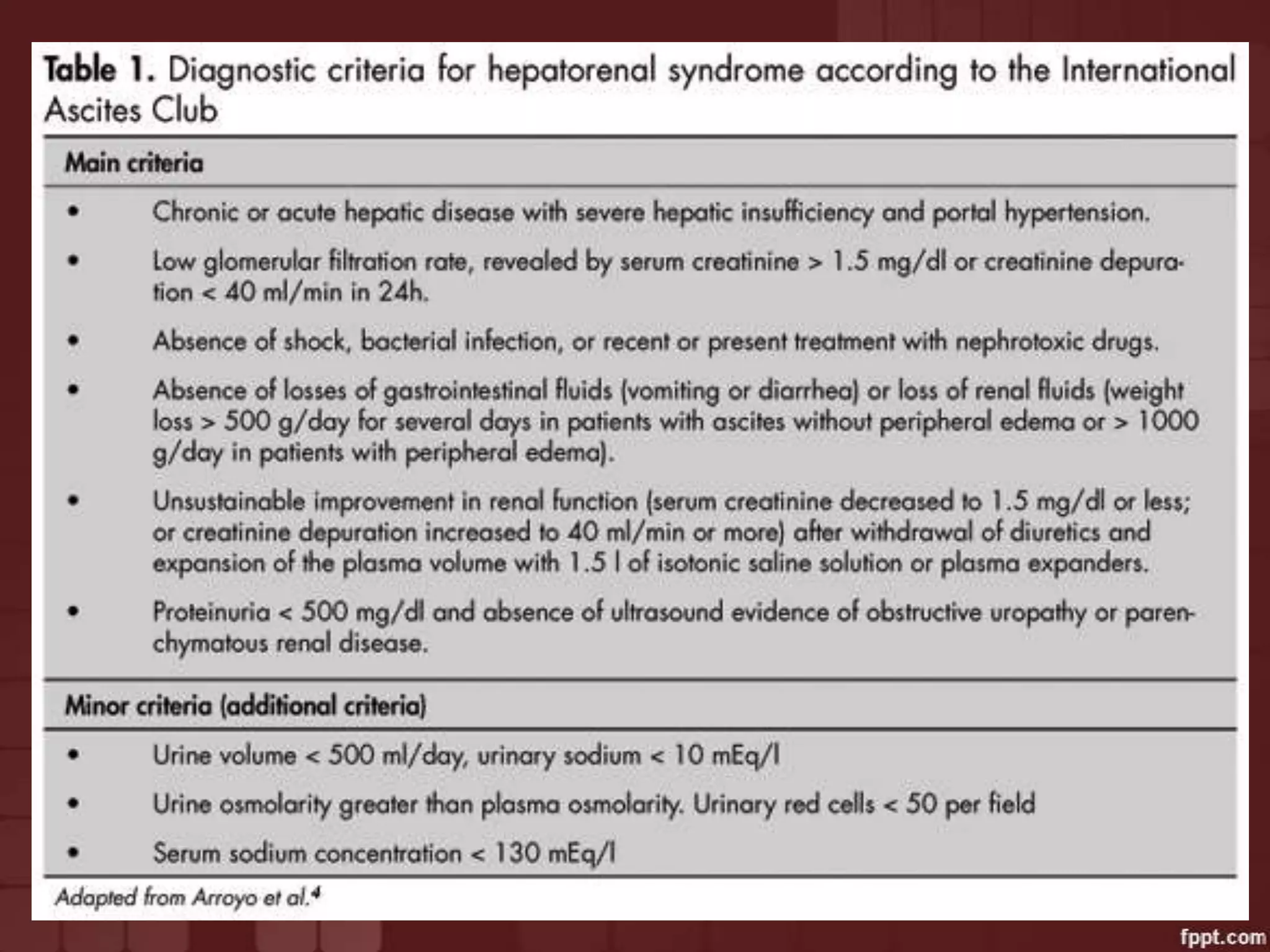

















































Hepato Renal Syndrome (HRS) is a form of kidney failure that occurs in patients with advanced chronic liver disease. It results from intense renal vasoconstriction caused by interactions between the systemic and portal circulatory systems. HRS has no underlying kidney pathology and typically develops spontaneously or in response to precipitating events like infections, bleeding, or large volume paracentesis. Diagnosis is based on criteria and HRS carries the worst prognosis of all liver disease complications. Treatment involves terlipressin and liver transplantation provides a definitive cure.