- Orthostatic hypotension is defined as a drop in blood pressure of at least 20 mm Hg systolic or 10 mm Hg diastolic within 3 minutes of standing.
- A tilt test evaluates a person's response to orthostatic stress by monitoring their heart rate and blood pressure as they are tilted from a lying to standing position. It is used to diagnose unexplained syncope.
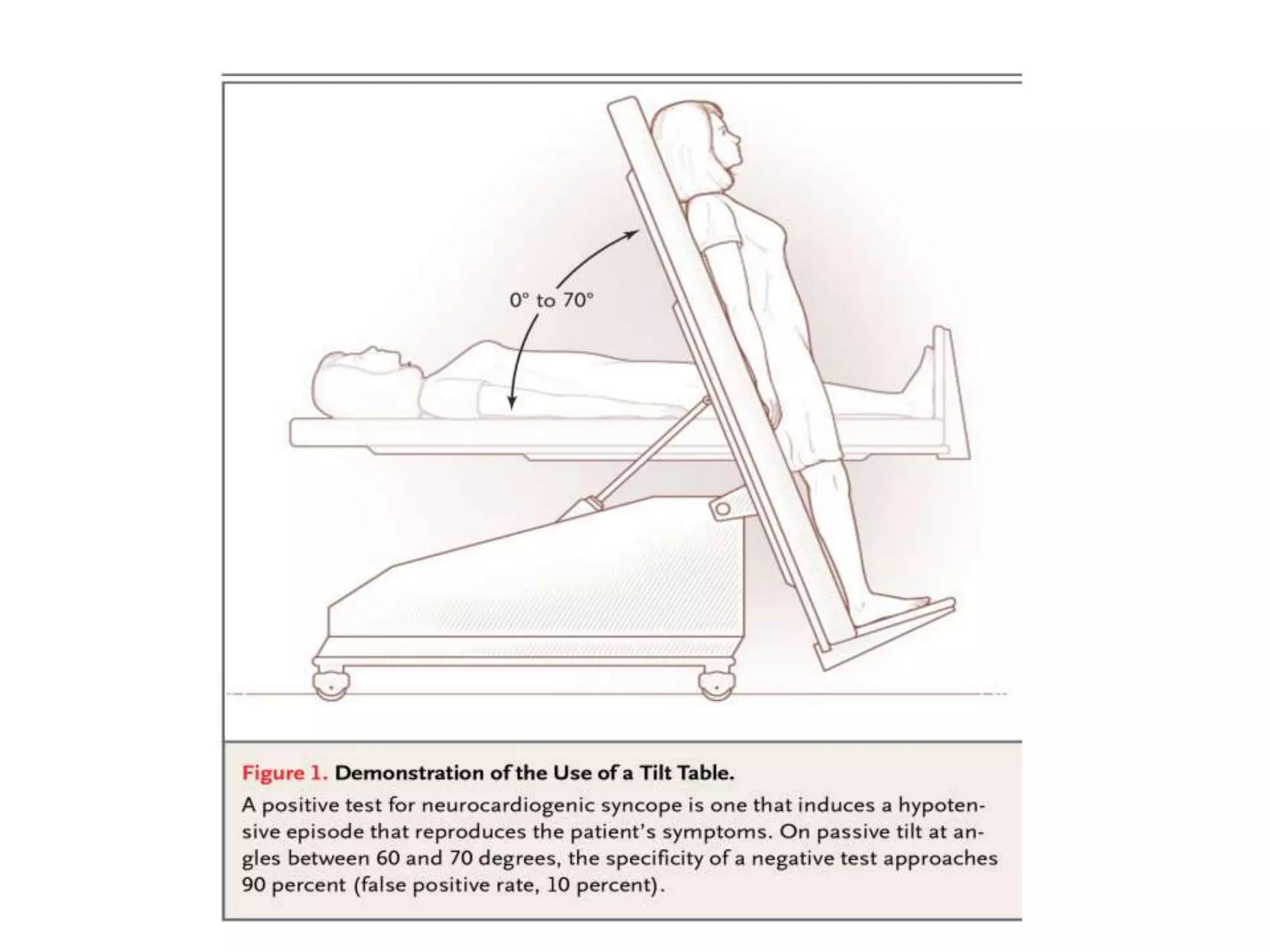
- The tilt test involves strapping a patient to a table that is tilted to different angles while their heart rate, blood pressure, oxygen levels and ECG are monitored for up to 45 minutes. A positive test result reproduces the patient's syncope symptoms along with hypotension, bradycardia or both