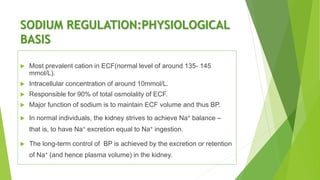
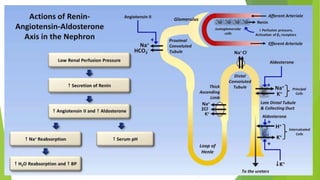
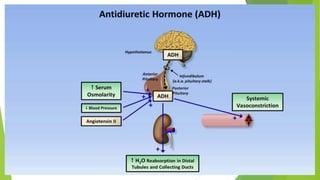
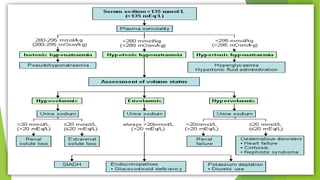
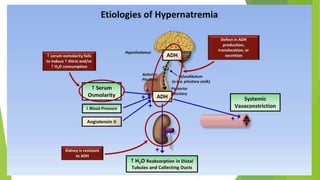
This document discusses hyponatremia and hypernatremia. It begins by explaining sodium regulation and the physiological basis of serum sodium concentration. It then defines and describes the types and causes of hyponatremia, including hypovolemic, euvolemic, and hypervolemic hyponatremia as well as pseudo hyponatremia. Specific conditions like SIADH are explained in detail. The clinical features, diagnosis, and treatment of hyponatremia are outlined. Hypernatremia is also defined and the causes of net water loss and hypertonic sodium gain are listed. The clinical features of hypernatremia are said to be predominantly neurologic.