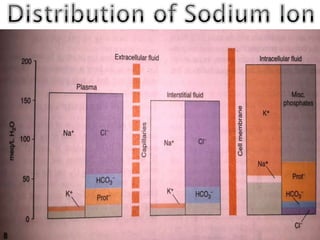
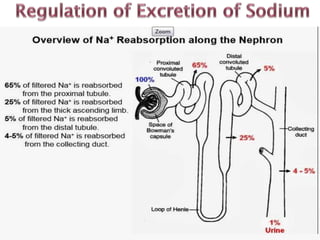
Sodium is the most abundant cation in extracellular fluid and accounts for 90% of plasma osmotic activity. Normal sodium levels are 130-145 mEq/L. Hyponatremia is defined as sodium <130 mEq/L and is classified as mild, moderate or severe based on sodium levels. Hypernatremia is defined as sodium >145 mEq/L. Causes, clinical features, and management of hypo- and hypernatremia are discussed. Slow correction of sodium levels is important to avoid complications.