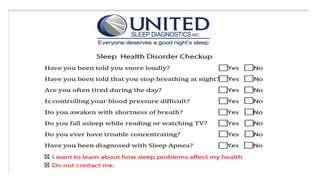
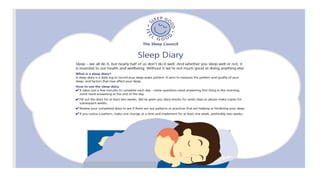
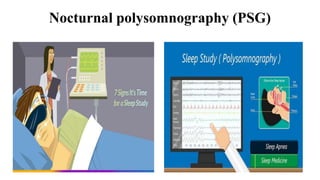
This document discusses sleep patterns and sleep disturbances. It begins by defining sleep and describing the sleep-wake cycle which is regulated by circadian rhythms. It then outlines the stages of sleep including non-REM and REM sleep. Key factors that affect sleep like age, illness, lifestyle and environment are mentioned. Common sleep disorders are introduced including insomnia, narcolepsy, sleep apnea, and parasomnias. Assessment methods like questionnaires, sleep diaries and polysomnography are covered. Nursing management strategies to promote better sleep are provided. Research evidence on sleep enhancement interventions for hospitalized patients is briefly summarized.


![Sleep pattern and its
disturbance
Evaluator: Dr Mahalingham V Presenter: Shruti Shirke
[Asst. professor, CON AIIMS BBSR] M.Sc Neuroscience Nursing](https://image.slidesharecdn.com/sleeppatterndisturbances-210806045903/85/Sleep-pattern-disturbances-2-320.jpg)




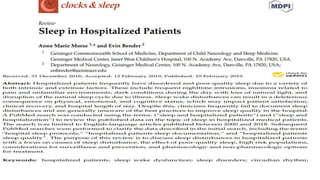


![Reference: cont..
• Surekha Anbazhagan, Naveen Ramesh, Catherine Nisha, Bobby Joseph Indian
Environ Med. 2016 Jan-Apr; 20(1): 35–38. doi: 10.4103/0019-5278.183842
PMCID: PMC4922274
• https://www.sccm.org/ICULiberation/Resources/PADIS-Guidelines-
Teaching-Slides-Sleep
• Pisani MA, Friese RS, Gehlbach BK, et al. Sleep in the intensive care
unit. Am J Respir Crit Care Med. 2015;191:731–738. [PMC free
article] [PubMed] [Google Scholar]](https://image.slidesharecdn.com/sleeppatterndisturbances-210806045903/85/Sleep-pattern-disturbances-64-320.jpg)














































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)








