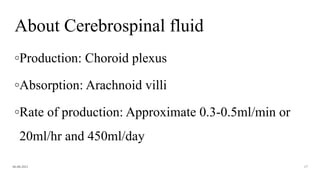
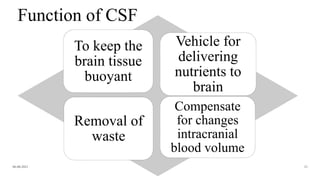
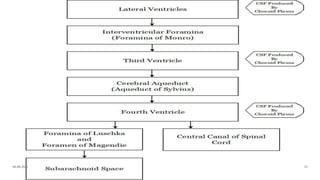
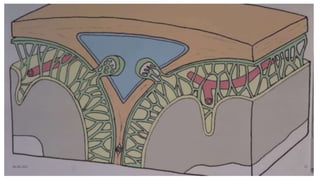
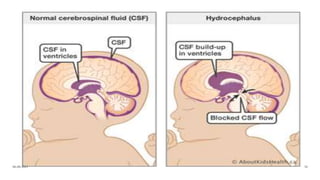
The document discusses hydrocephalus, including its definition, anatomy, types, causes, signs and symptoms, diagnosis, and management. Hydrocephalus is a condition caused by an imbalance in CSF production and absorption, leading to ventricular enlargement. It can be congenital or acquired. Types include communicating, non-communicating, and normal pressure hydrocephalus. Management involves medical treatment or surgical options like shunting procedures or endoscopic third ventriculostomy. An external ventricular drain (EVD) may be used to temporarily treat hydrocephalus by draining excess CSF.
![HYDROCEPHALUS
Evaluator: Mr L Anand Presenter: Shruti Shirke
[Asso professor, CON AIIMS BBSR] M.Sc Neuroscience Nursing
06-08-2021
1](https://image.slidesharecdn.com/hydrocephalusautosaved-210806045751/85/Hydrocephalus-1-320.jpg)
![HYDROCEPHALUS
Evaluator: Mr L Anand Presenter: Shruti Shirke
[Asso professor, CON AIIMS BBSR] M.Sc Neuroscience Nursing
06-08-2021
1](https://image.slidesharecdn.com/hydrocephalusautosaved-210806045751/75/Hydrocephalus-1-2048.jpg)







![◦ Humphrey E (2018) Caring for neurosurgical patients with external ventricular drains. Nursing Times
[online]; 114: 4, 52-56.
06-08-2021 78](https://image.slidesharecdn.com/hydrocephalusautosaved-210806045751/85/Hydrocephalus-78-320.jpg)
























































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)