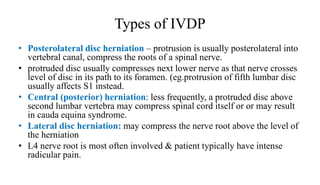
Intervertebral disc prolapse occurs when a tear in the outer ring of an intervertebral disc allows the central portion to bulge out. It most commonly affects the lumbar region. Symptoms include back pain radiating into the legs with numbness and tingling. Diagnosis involves imaging tests like MRI. Treatment options range from conservative measures like physical therapy to surgical procedures like discectomy. Nursing care focuses on pain management, proper body mechanics, exercise, and health education to prevent future episodes.
![INTERVERTEBRAL DISC
PROLAPSE
( IVDP)
Evaluator: Mr L Anand Presenter: Shruti Shirke
[Asso professor, CON AIIMS BBSR] M.Sc Neuroscience Nursing](https://image.slidesharecdn.com/ivdp-210806045752/85/Inter-vertebral-disc-prolapse-1-320.jpg)