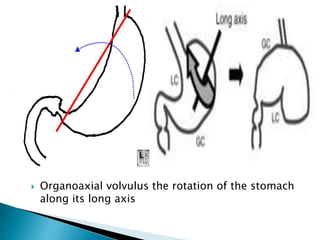
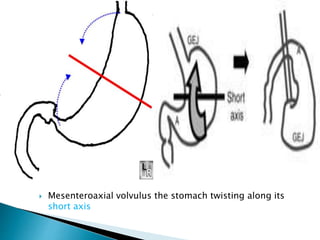
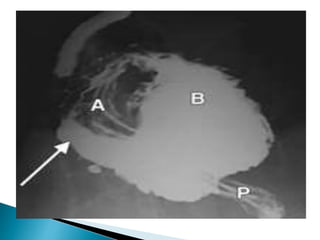
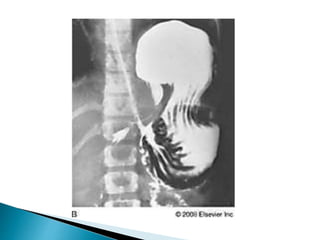
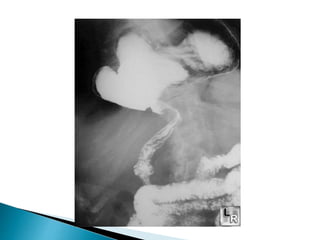
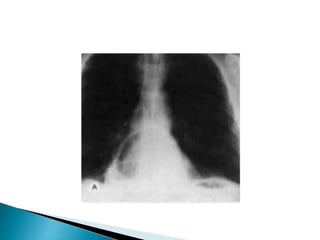
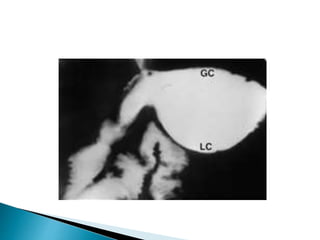
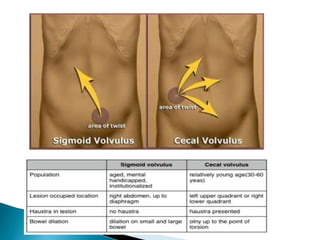
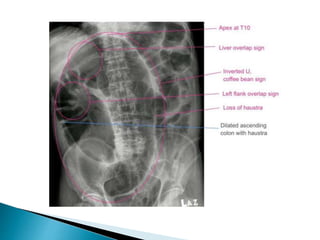
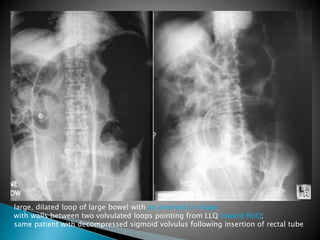
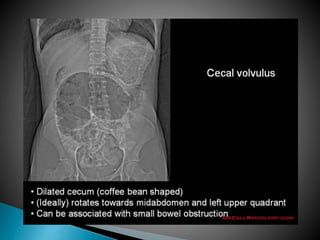
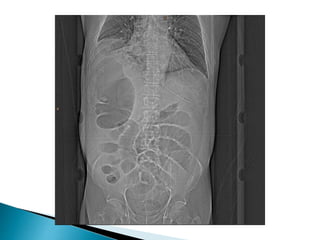
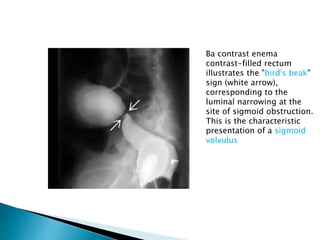
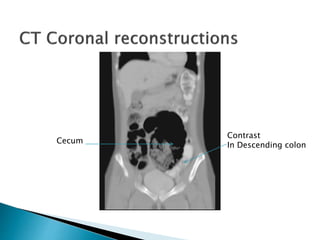
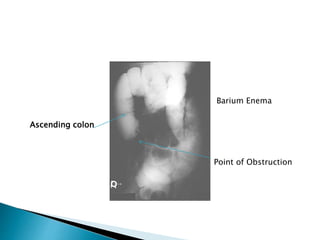
The document discusses different types of intestinal volvulus including gastric, small bowel, large bowel, and combinations. Gastric volvulus is classified as organoaxial or mesenteroaxial depending on the axis of rotation. Small bowel volvulus often occurs due to midgut malrotation. Large bowel volvulus commonly affects the cecum or sigmoid colon. Sigmoid volvulus is the most common type of large bowel volvulus and presents as an inverted U-shape on imaging. Cecal volvulus results from torsion of the cecum around its own mesentery.















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
















