Downloaded 79 times


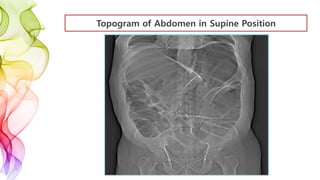
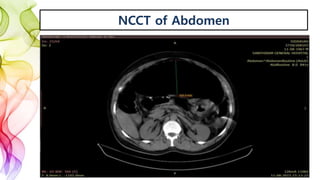
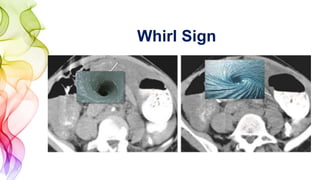













This document presents a case report of a 48-year-old male patient who presented with abdominal pain, distension, and constipation for 5 days. Imaging revealed a transverse colon volvulus, which was confirmed during surgery. Transverse colon volvulus is rare, accounting for only 2-4% of colonic volvulus cases. It carries a higher risk of mortality and morbidity than sigmoid or cecal volvulus. Prompt diagnosis through imaging and emergency surgical intervention is key to successful treatment outcomes.































































































