Downloaded 4,483 times




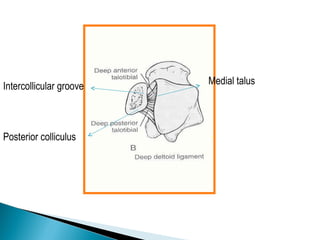






















![GOAL: TO EVALUATE DEEP DELTOID [i.e. INSTABILITY]
METHOD: MEDIAL TENDERNESS
MEDIAL SWELLING
MEDIAL ECCHYMOSIS
STRESS VIEWS- GRAVITY OR MANUAL](https://image.slidesharecdn.com/anklefracturesfinal-120314092959-phpapp01/85/Ankle-fractures-final-44-320.jpg)






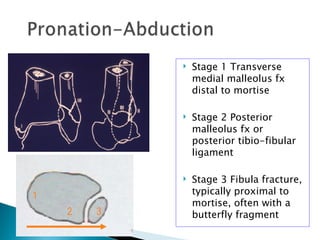
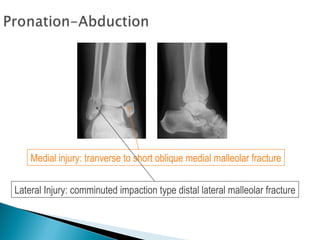

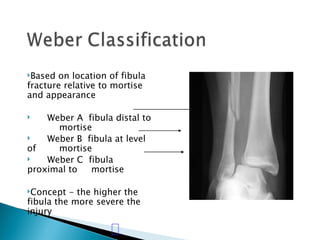


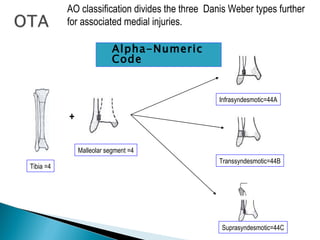
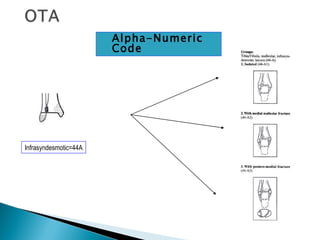




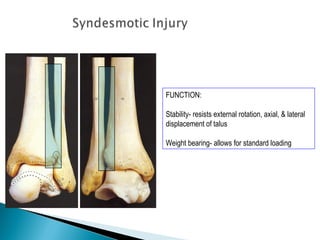












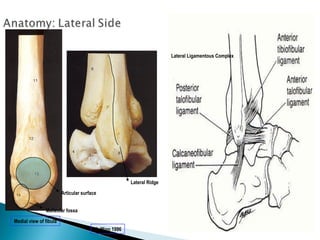
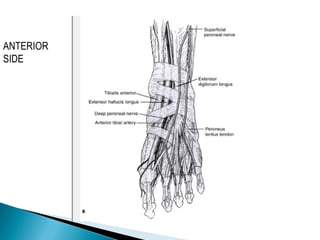
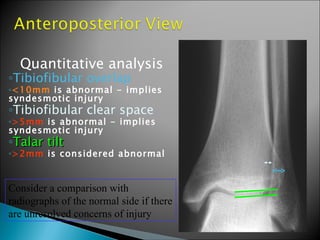
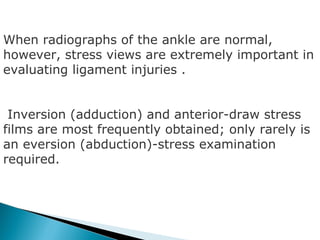
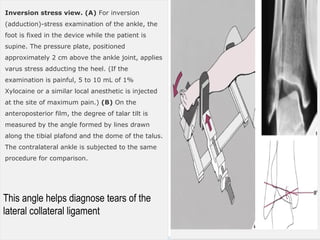
The document discusses the anatomy and biomechanics of the ankle joint. It describes the ankle joint as a three bone joint composed of the tibia, fibula, and talus. It notes that the talus articulates superiorly with the tibial plafond and posteriorly with the posterior malleolus of the tibia. The lateral articulation is with the malleolus of the fibula. The joint is saddle-shaped and wider anteriorly to accommodate dorsiflexion. Disruption of the ankle mortise can decrease contact area by 42%.