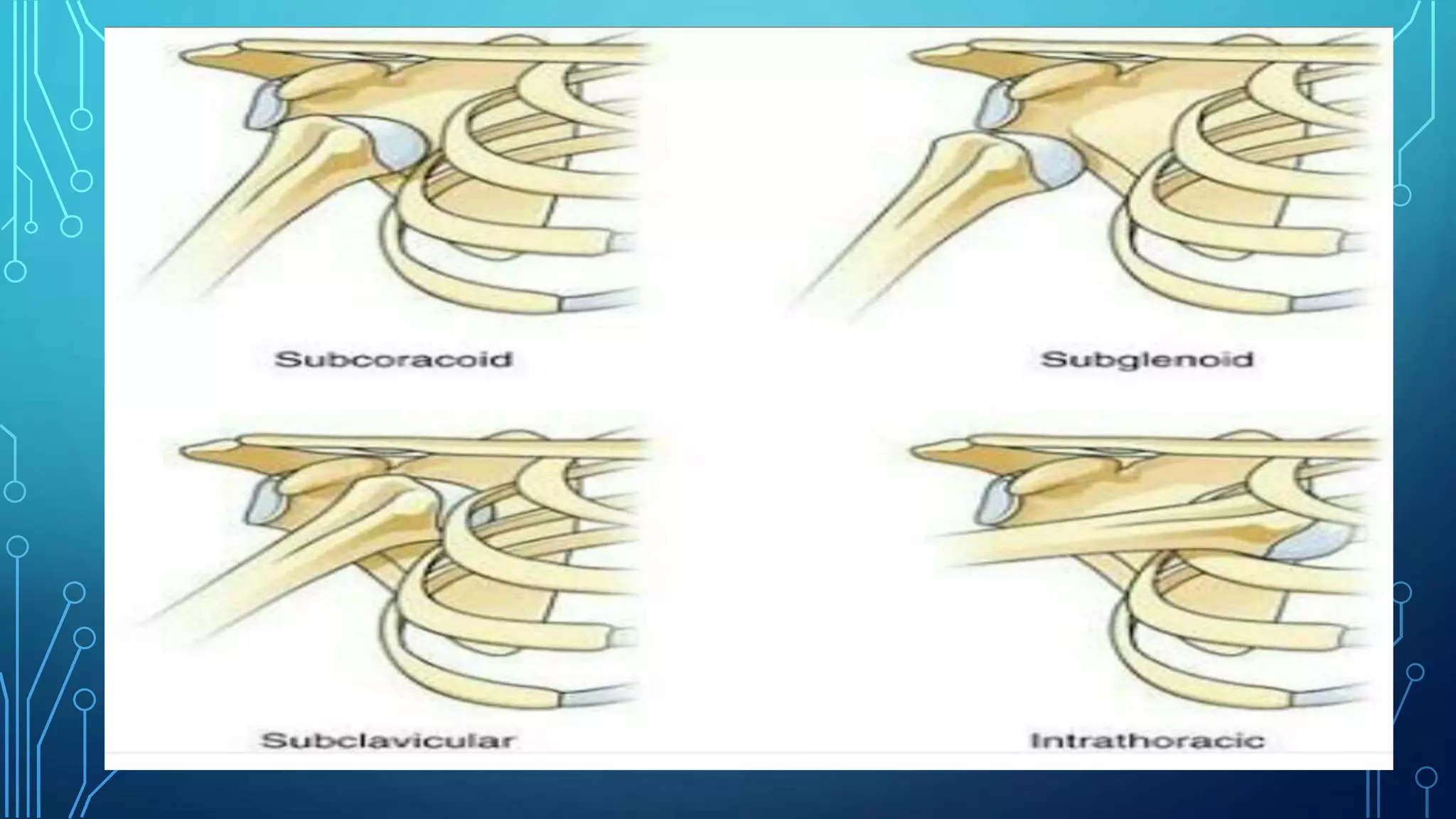
The document summarizes the types, diagnosis, treatment, and physiotherapy management of shoulder dislocations. There are three main types of shoulder dislocations - anterior, posterior, and luxatio erecta. Anterior dislocations are the most common, often caused by a fall on an outstretched hand. Treatment involves reduction, immobilization for 3 weeks, followed by a mobilization phase and physiotherapy to regain full range of motion. Physiotherapy focuses on strengthening muscles around the shoulder and regaining passive range of motion to prevent recurrent dislocations and return to full function.