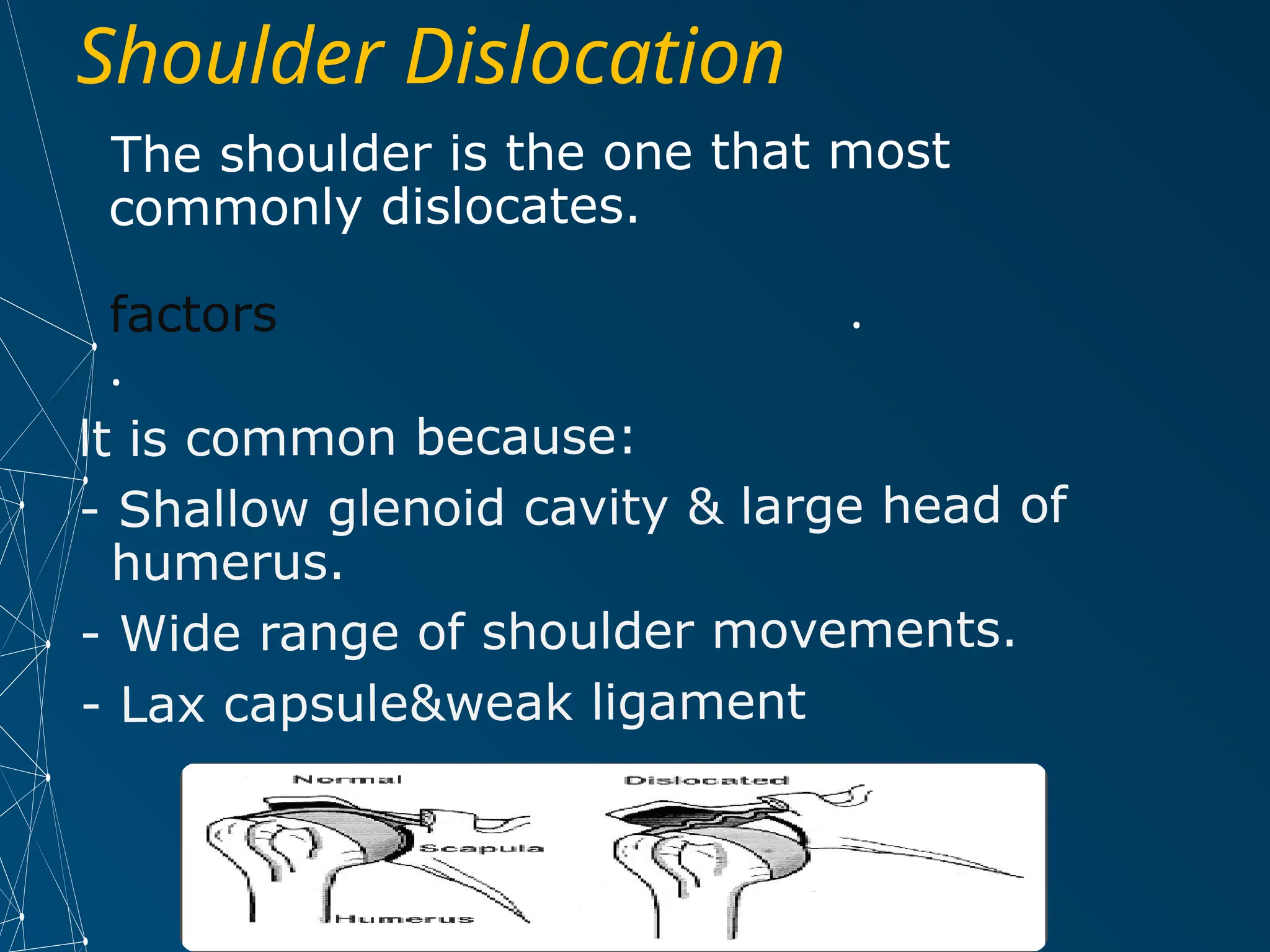
The document provides a comprehensive overview of shoulder joint dislocation, including anatomy, classification, clinical features, and management. It discusses various types of dislocations—anterior, posterior, and inferior—along with their causes, symptoms, and treatment methods. Additionally, it highlights potential complications associated with shoulder dislocations and injuries to the acromioclavicular joint.