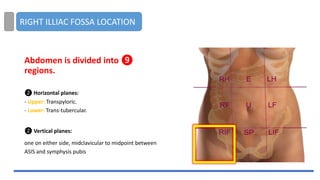
Abdomen is dividedinto ❾
regions.
❷ Horizontal planes:
- Upper: Transpyloric.
- Lower: Trans-tubercular.
❷ Vertical planes:
one on either side, midclavicular to midpoint between
ASIS and symphysis pubis
RIGHT ILLIAC FOSSA LOCATION
3.
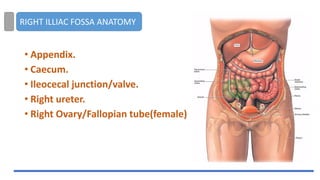
• Appendix.
• Caecum.
•Ileocecal junction/valve.
• Right ureter.
• Right Ovary/Fallopian tube(female)
RIGHT ILLIAC FOSSA ANATOMY
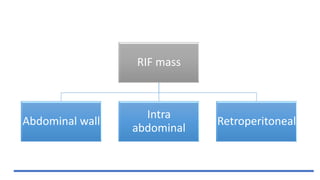
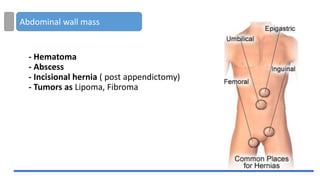
Abdominal wall mass
-Hematoma
- Abscess
- Incisional hernia ( post appendictomy)
- Tumors as Lipoma, Fibroma
6.
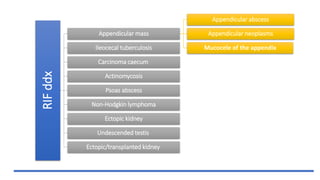
RIF
ddx
Appendicular mass
Appendicular abscess
Appendicularneoplasms
Mucocele of the appendix
Ileocecal tuberculosis
Carcinoma caecum
Actinomycosis
Psoas abscess
Non-Hodgkin lymphoma
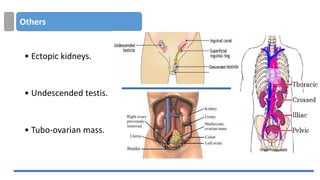
Ectopic kidney
Undescended testis
Ectopic/transplanted kidney
7.
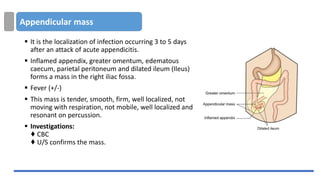
Appendicular mass
▪ Itis the localization of infection occurring 3 to 5 days
after an attack of acute appendicitis.
▪ Inflamed appendix, greater omentum, edematous
caecum, parietal peritoneum and dilated ileum (Ileus)
forms a mass in the right iliac fossa.
▪ Fever (+/-)
▪ This mass is tender, smooth, firm, well localized, not
moving with respiration, not mobile, well localized and
resonant on percussion.
▪ Investigations:
♦ CBC
♦ U/S confirms the mass.
8.
Appendicular mass
▪ Treatment:
▪Conservative (Ochsner-Sherren Regimen),
Includes:
▪ Temp, BP, pulse chart, marking the
(progression/regression).
▪ Antibiotics (Ampicillin, metronidazole), IV fluids
and analgesics.
▪ Contraindications for Ochsner-Sherren regimen:
1. When diagnosis is in doubt.
2. In acute appendicitis in children and elderly.
3. Gangrenous appendicitis.
4. Diffuse peritonitis sets in.
9.
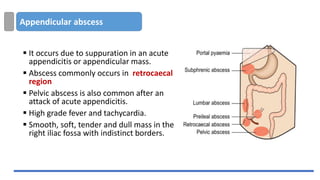
Appendicular abscess
▪ Itoccurs due to suppuration in an acute
appendicitis or appendicular mass.
▪ Abscess commonly occurs in retrocaecal
region
▪ Pelvic abscess is also common after an
attack of acute appendicitis.
▪ High grade fever and tachycardia.
▪ Smooth, soft, tender and dull mass in the
right iliac fossa with indistinct borders.
10.
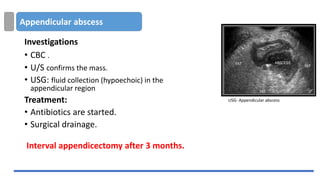
Appendicular abscess
Investigations
• CBC.
• U/S confirms the mass.
• USG: fluid collection (hypoechoic) in the
appendicular region
Treatment:
• Antibiotics are started.
• Surgical drainage.
Interval appendicectomy after 3 months.
USG- Appendicular abscess
11.
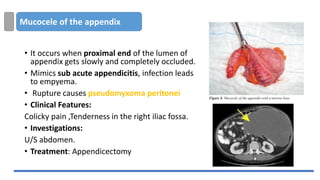
Mucocele of theappendix
• It occurs when proximal end of the lumen of
appendix gets slowly and completely occluded.
• Mimics sub acute appendicitis, infection leads
to empyema.
• Rupture causes pseudomyxoma peritonei
• Clinical Features:
Colicky pain ,Tenderness in the right iliac fossa.
• Investigations:
U/S abdomen.
• Treatment: Appendicectomy
12.
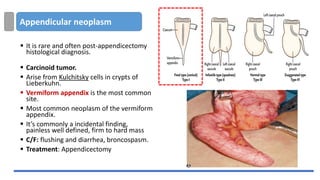
Appendicular neoplasm
▪ Itis rare and often post-appendicectomy
histological diagnosis.
▪ Carcinoid tumor.
▪ Arise from Kulchitsky cells in crypts of
Lieberkuhn.
▪ Vermiform appendix is the most common
site.
▪ Most common neoplasm of the vermiform
appendix.
▪ It’s commonly a incidental finding,
painless well defined, firm to hard mass
▪ C/F: flushing and diarrhea, broncospasm.
▪ Treatment: Appendicectomy
13.
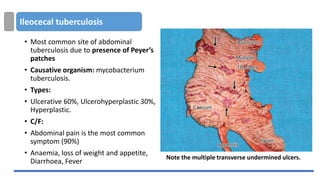
Ileocecal tuberculosis
• Mostcommon site of abdominal
tuberculosis due to presence of Peyer’s
patches
• Causative organism: mycobacterium
tuberculosis.
• Types:
• Ulcerative 60%, Ulcerohyperplastic 30%,
Hyperplastic.
• C/F:
• Abdominal pain is the most common
symptom (90%)
• Anaemia, loss of weight and appetite,
Diarrhoea, Fever
Note the multiple transverse undermined ulcers.
14.
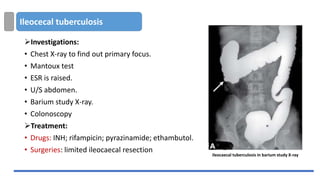
Ileocecal tuberculosis
➢Investigations:
• ChestX-ray to find out primary focus.
• Mantoux test
• ESR is raised.
• U/S abdomen.
• Barium study X-ray.
• Colonoscopy
➢Treatment:
• Drugs: INH; rifampicin; pyrazinamide; ethambutol.
• Surgeries: limited ileocaecal resection
ileocaecal tuberculosis in barium study X-ray
15.
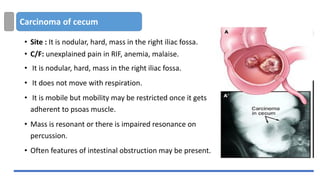
Carcinoma of cecum
•Site : It is nodular, hard, mass in the right iliac fossa.
• C/F: unexplained pain in RIF, anemia, malaise.
• It is nodular, hard, mass in the right iliac fossa.
• It does not move with respiration.
• It is mobile but mobility may be restricted once it gets
adherent to psoas muscle.
• Mass is resonant or there is impaired resonance on
percussion.
• Often features of intestinal obstruction may be present.
16.
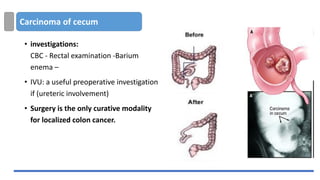
Carcinoma of cecum
•investigations:
CBC - Rectal examination -Barium
enema –
• IVU: a useful preoperative investigation
if (ureteric involvement)
• Surgery is the only curative modality
for localized colon cancer.
17.
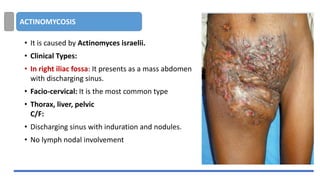
ACTINOMYCOSIS
• It iscaused by Actinomyces israelii.
• Clinical Types:
• In right iliac fossa: It presents as a mass abdomen
with discharging sinus.
• Facio-cervical: It is the most common type
• Thorax, liver, pelvic
C/F:
• Discharging sinus with induration and nodules.
• No lymph nodal involvement
18.
ACTINOMYCOSIS
• Investigations
• Pusunder microscopy shows branching filaments.
• Gram’s staining shows Gram-positive mycelia
• Treatment
• Penicillin G for longer period (6-12 weeks).
• Surgical debridement is occasionally required.
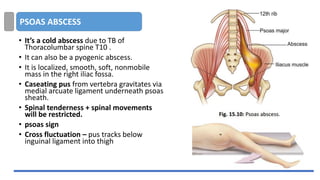
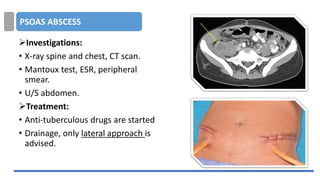
PSOAS ABSCESS
• It’sa cold abscess due to TB of
Thoracolumbar spine T10 .
• It can also be a pyogenic abscess.
• It is localized, smooth, soft, nonmobile
mass in the right iliac fossa.
• Caseating pus from vertebra gravitates via
medial arcuate ligament underneath psoas
sheath.
• Spinal tenderness + spinal movements
will be restricted.
• psoas sign
• Cross fluctuation – pus tracks below
inguinal ligament into thigh
21.
PSOAS ABSCESS
➢Investigations:
• X-rayspine and chest, CT scan.
• Mantoux test, ESR, peripheral
smear.
• U/S abdomen.
➢Treatment:
• Anti-tuberculous drugs are started
• Drainage, only lateral approach is
advised.
22.
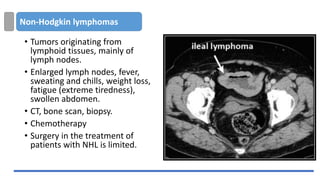
Non-Hodgkin lymphomas
• Tumorsoriginating from
lymphoid tissues, mainly of
lymph nodes.
• Enlarged lymph nodes, fever,
sweating and chills, weight loss,
fatigue (extreme tiredness),
swollen abdomen.
• CT, bone scan, biopsy.
• Chemotherapy
• Surgery in the treatment of
patients with NHL is limited.
Question and answer:
•Appendicularabscess commonly
occurs in which region:
1. Subcaecal
2. Retrocaecal
3. Preileal lumbar
4. Postileal regions
25.
Question and answer:
•Appendicularabscess commonly
occurs in which region:
1. Subcaecal
2.Retrocaecal
3. Preileal lumbar
4. Postileal regions
26.
Question and answer:
•Drugof choice for treating infections
caused by actinomycetes ?
a) Amphotericin B
b) Co-trimoxazole
c) Penicillin
d) Itraconazole
27.
Question and answer:
•Drugof choice for treating infections
caused by actinomycetes ?
a) Amphotericin B
b) Co-trimoxazole
c) Penicillin
d) Itraconazole