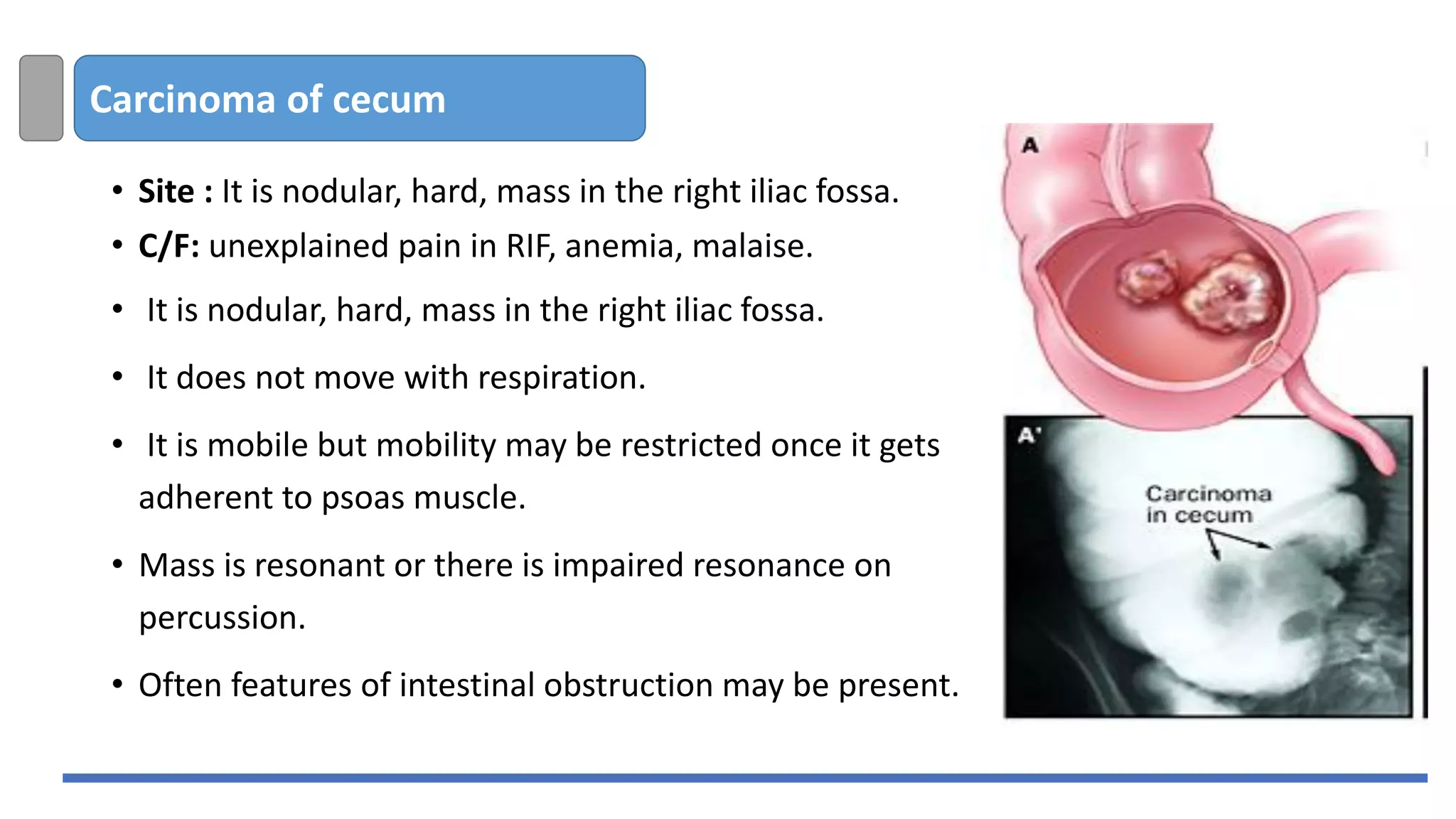
The document provides a comprehensive overview of right iliac fossa masses, detailing anatomical locations, differential diagnoses, clinical features, investigations, and treatment strategies for conditions such as appendicular masses, abscesses, tumors, and infections like ileocecal tuberculosis and actinomycosis. It discusses specific cases including appendicitis, mucocele of the appendix, and non-Hodgkin lymphoma, along with treatment options ranging from conservative management to surgical intervention. Various diagnostic methods, including ultrasound and imaging studies, are highlighted for accurate assessment.