Downloaded 164 times

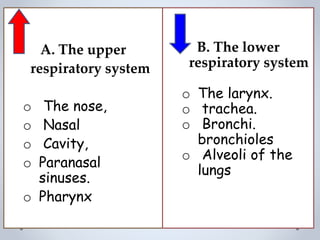
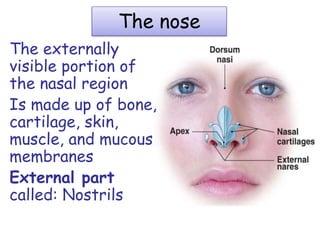
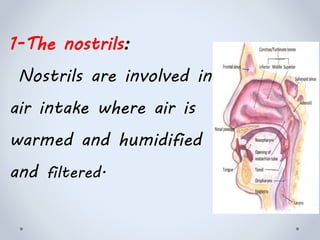
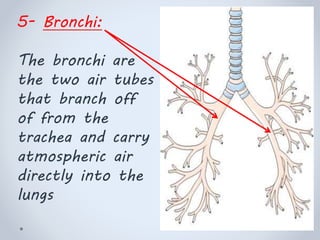
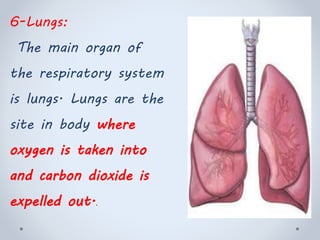
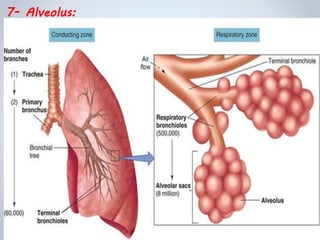
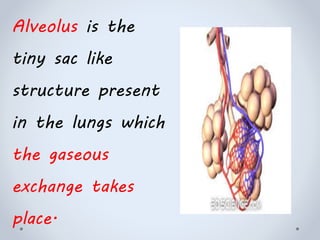
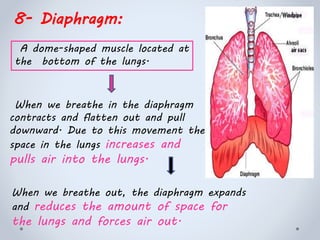

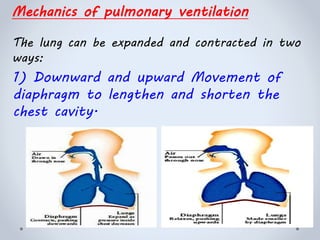
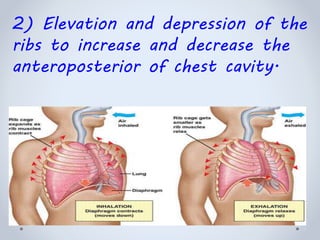
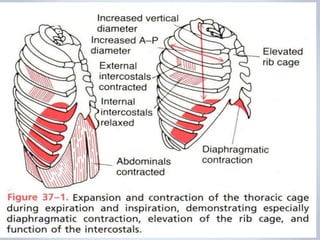



The document summarizes the structure and function of the respiratory system. It describes the major parts including the nose, pharynx, larynx, trachea, bronchi, lungs and alveoli. It explains how breathing works through the contraction of the diaphragm and movement of the ribs. Gas exchange occurs in the alveoli through diffusion. Various pressures and volumes related to breathing are also defined. Pulmonary ventilation involves the inflow and outflow of air and is regulated by the nervous system and local factors.