Download to read offline
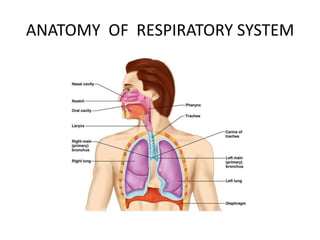
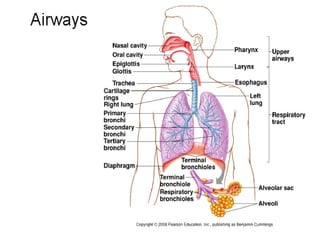
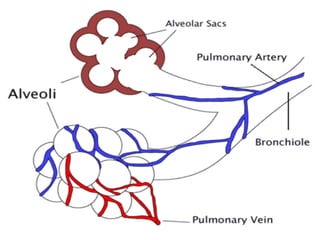
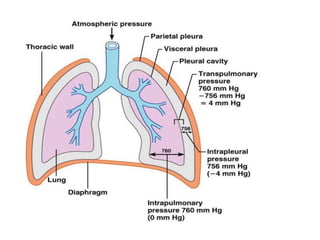
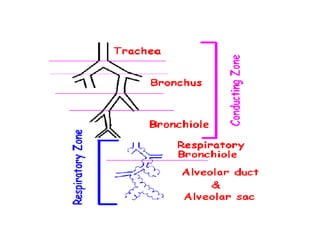
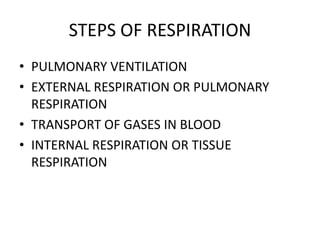
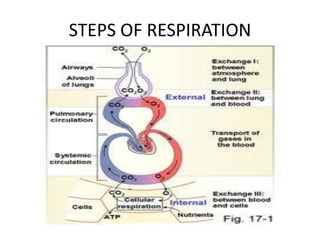
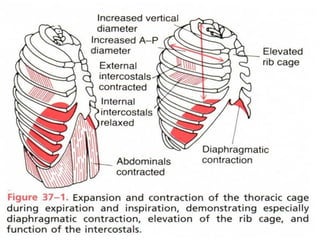
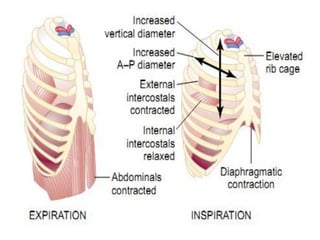
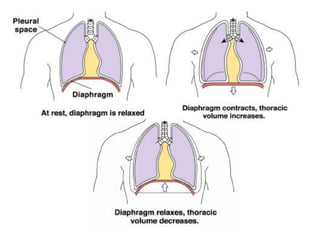
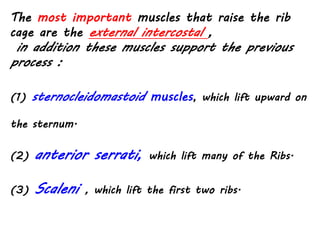
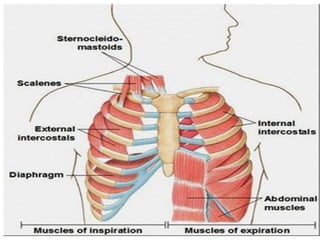
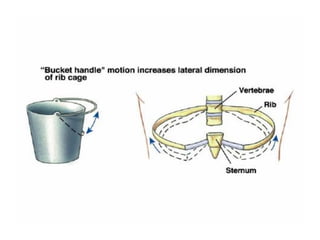
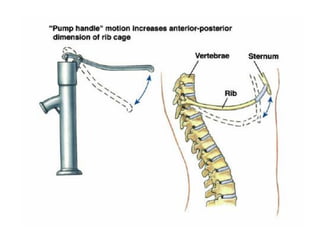
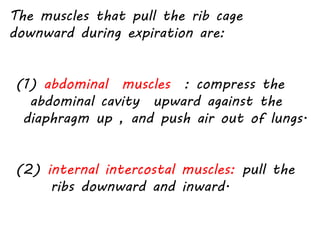
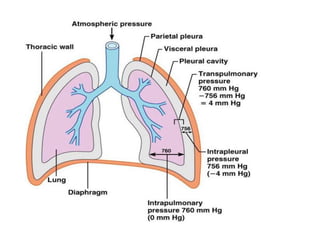
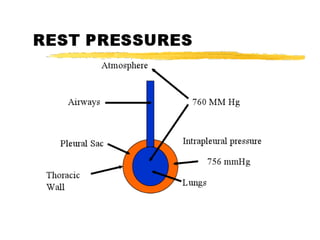
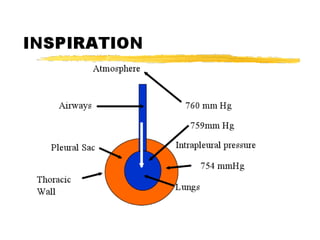
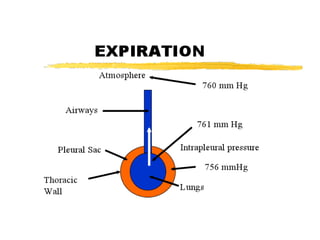
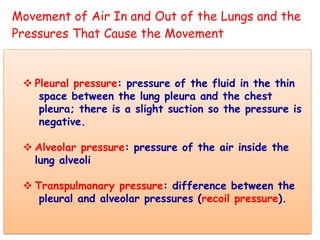
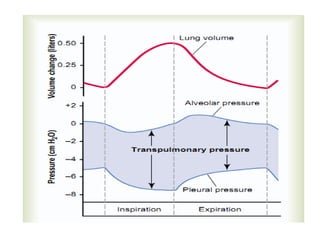


This document discusses the mechanism of respiration including: 1) It describes the anatomy of the respiratory system including the pleura, lungs, and pressures involved. 2) It explains the stages of respiration including pulmonary ventilation, gas exchange in the lungs and blood, and tissue respiration. 3) It details the mechanics of breathing involving the muscles that cause inhalation and exhalation and how pressures change in the lungs and chest.















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)






