Downloaded 152 times

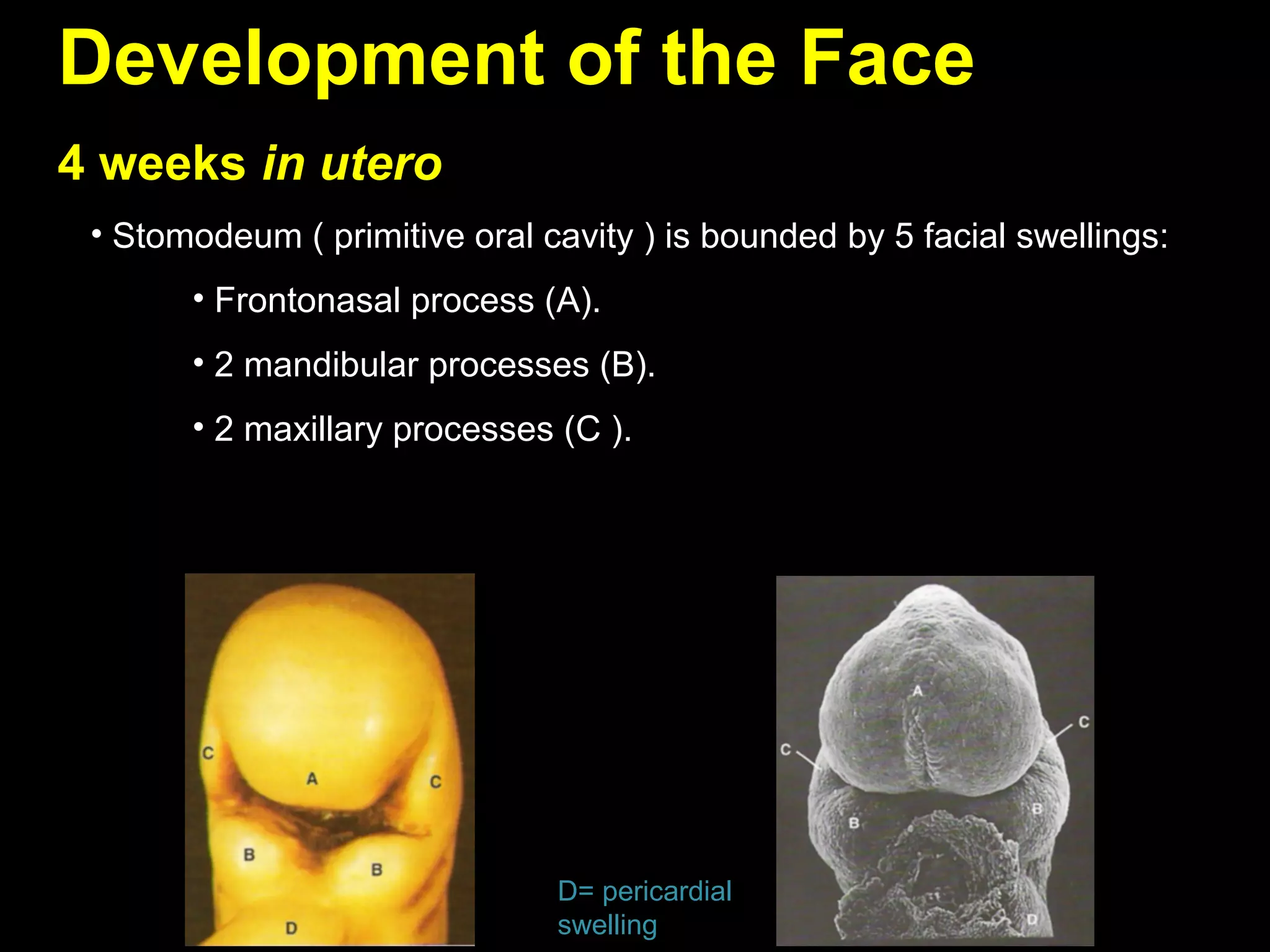




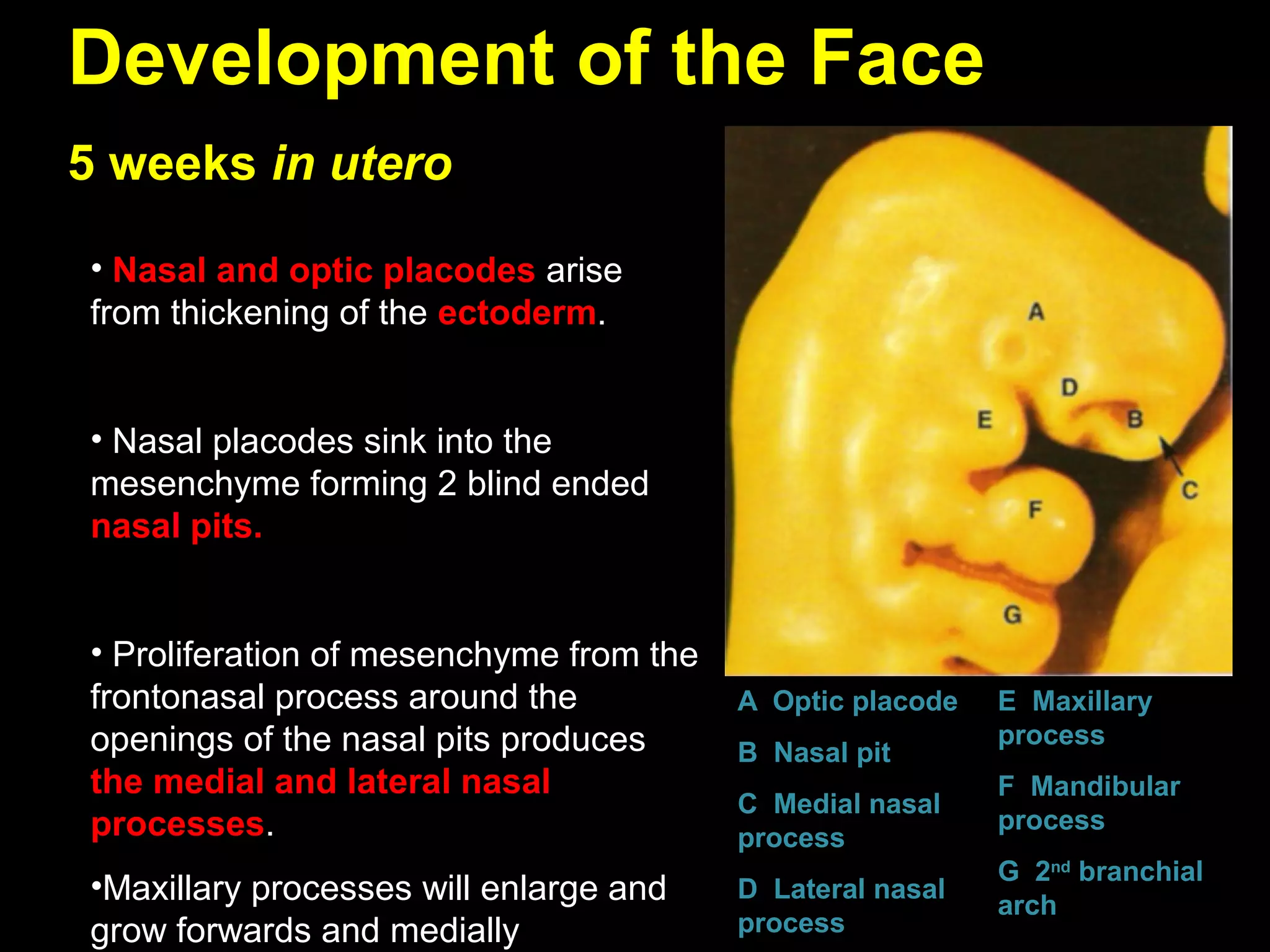











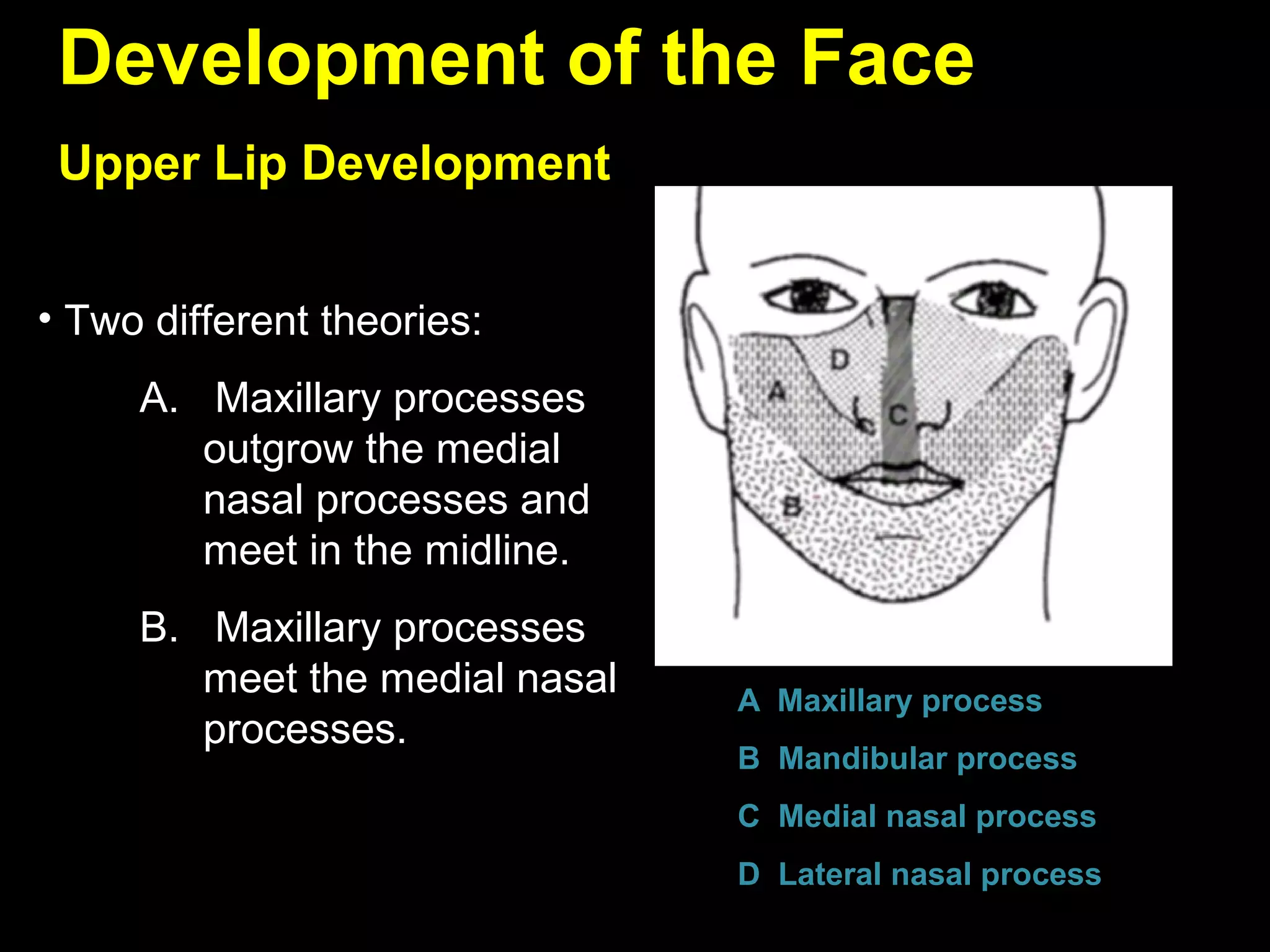





































The document describes the development of various facial structures in utero from 4-12 weeks gestation. It discusses how the frontonasal process, mandibular processes, and maxillary processes give rise to the primitive oral cavity and facial swellings at 4 weeks. By 5 weeks, the nasal pits have formed and the oronasal membranes separate the nasal and oral cavities. By 6 weeks, fusion of the mandibular processes occurs and palatal shelves begin to develop from the maxillary processes. Between 8-12 weeks, the palatal shelves fuse to form the secondary palate separating the oral and nasal cavities. The development of other structures like the mandible, maxilla, tongue are also described.

























































![PRE-NATAL GRnnnmnnnnmmOWTH seminar[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/pre-natalgrowthseminar1-250427093235-de04befc-thumbnail.jpg?width=640&height=640&fit=bounds)

















































