Nose
External nose –portion visible on face
The interior structures of the external nose have three functions:
• warming, moistening, and filtering incoming air;
• detecting olfactory stimuli;
• modifying speech vibrations as they pass through the large, hollow resonating
chambers.
Internal nose – large cavity beyond nasal vestibule
• Internal nares or choanae
• Ducts from paranasal sinuses and nasolacrimal ducts open into internal nose
• Nasal cavity divided by nasal septum and subdivide cavity into meatuses: Increase
surface are and prevents dehydration
• Olfactory receptors in olfactory epithelium
4.
Cilia and mucus
Theepithelial surfaces of the airways, from nose to the lungs:
Ø contain cilia that transport the mucus to the pharynx
Ø Mucus are secreted by the goblet cells
Functions:
• Mucus is important to keep the lungs clear of particle matter and many bacteria that enter
the body on dust particles.
• warmed the air moving into body by the heat providing by the presence of the capillaries
5.
Each lung isenclosed and protected by a double-layered membrane known as the
pleural membrane:
The visceral pleura: covers the external surface of lung
The parietal pleura: covers the wall of the thoracic cavity
The pleural cavity: a space between the two layers,
contains a lubricating fluid (intrapleural fluid).
This pleural fluid reduces friction between
the membranes, allowing them to slide easily
over one another during breathing.
Lungs
6.
Functionally, the respiratorysystem consists of two parts:
1. Conducting zone – Filter, warm and conducts air to lungs
Nose, pharynx, larynx, trachea, bronchi, bronchioles and terminal bronchioles
Functions of the Respiratory System
7.
2. Respiratory zone– main site of gas exchange between air and blood
Respiratory bronchioles, alveolar ducts, alveolar sacs, and alveoli
Functions of the Respiratory System
Alveoli highly important for Gas Exchange
8.
Dr. Lina SABRA-MAKKE
Componentsof Alveolus
Lungs receive blood from
Pulmonary artery- deoxygenated blood
Bronchial arteries – oxygenated blood to perfuse the muscular walls of bronchi
and bronchioles
9.
a) Type Ialveolar cells:
• thin epithelial cells
•Make up most of the alveolar
walls
b) Type II alveolar cells:
• thick epithelial cells that
produce a detergent; Surfactant
c) Alveolar macrophages:
• phagocytosis and defense
The main types of alveolar cells
10.
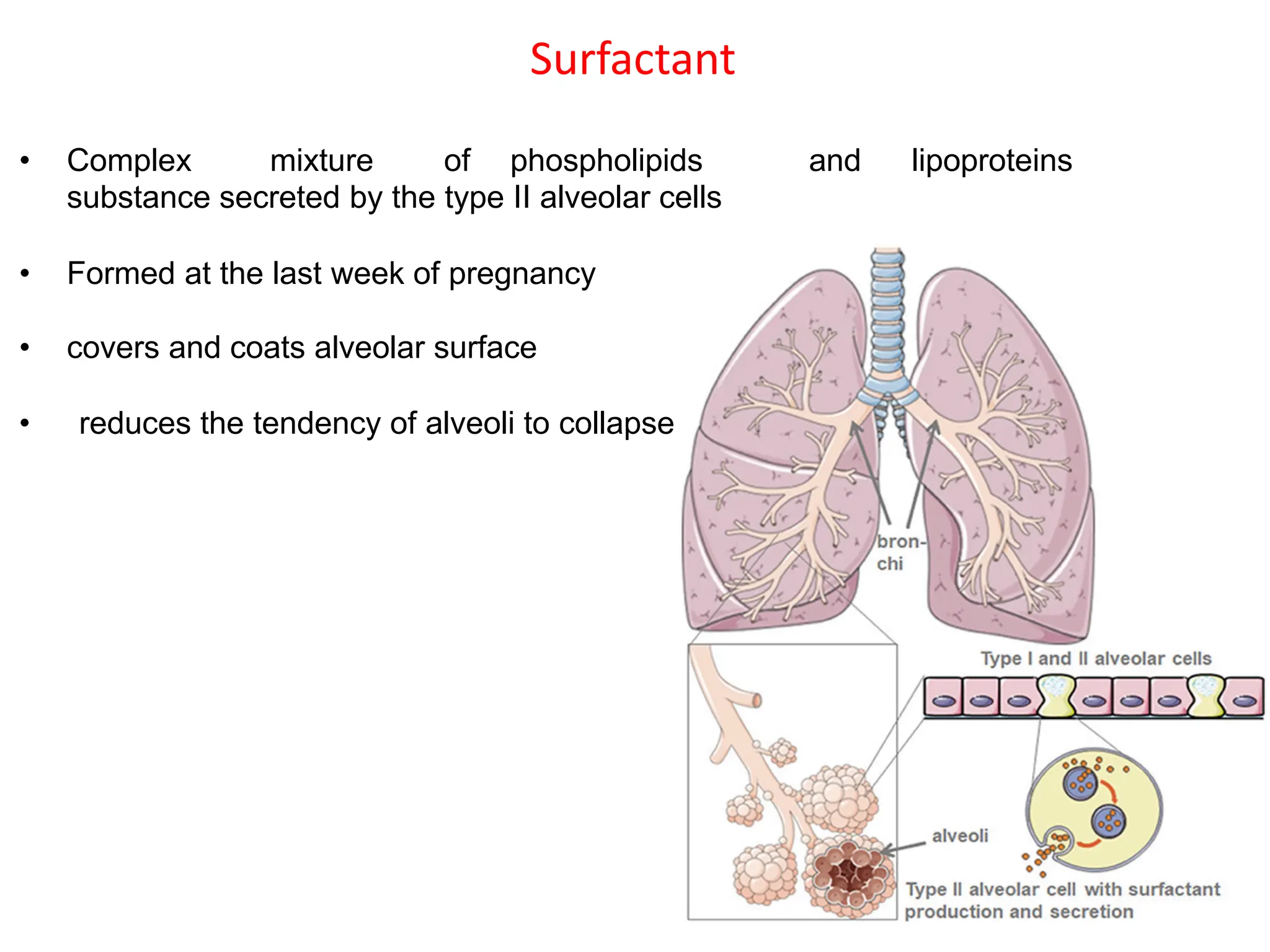
Surfactant
• Complex mixtureof phospholipids and lipoproteins
substance secreted by the type II alveolar cells
• Formed at the last week of pregnancy
• covers and coats alveolar surface
• reduces the tendency of alveoli to collapse
11.
• In thelungs we have two
major cholinergic and adrenergic
receptors subtypes: M3 cholinergic and
β2 adrenergic receptors
• Stimulation of M3 receptors causes
bronchoconstriction while the
stimulation of β2 receptors causes a
bronchodilation.
ü Its is useful to note that an asthma is a chronic inflammation of smooth
airways and is characterized by an intense broncho- constriction.
ü We used an adrenaline to calm this problem.
ü Thus, β2- adrenergic drugs (Ventolin: Salbutamol) are used in the treatment
of asthma
12.
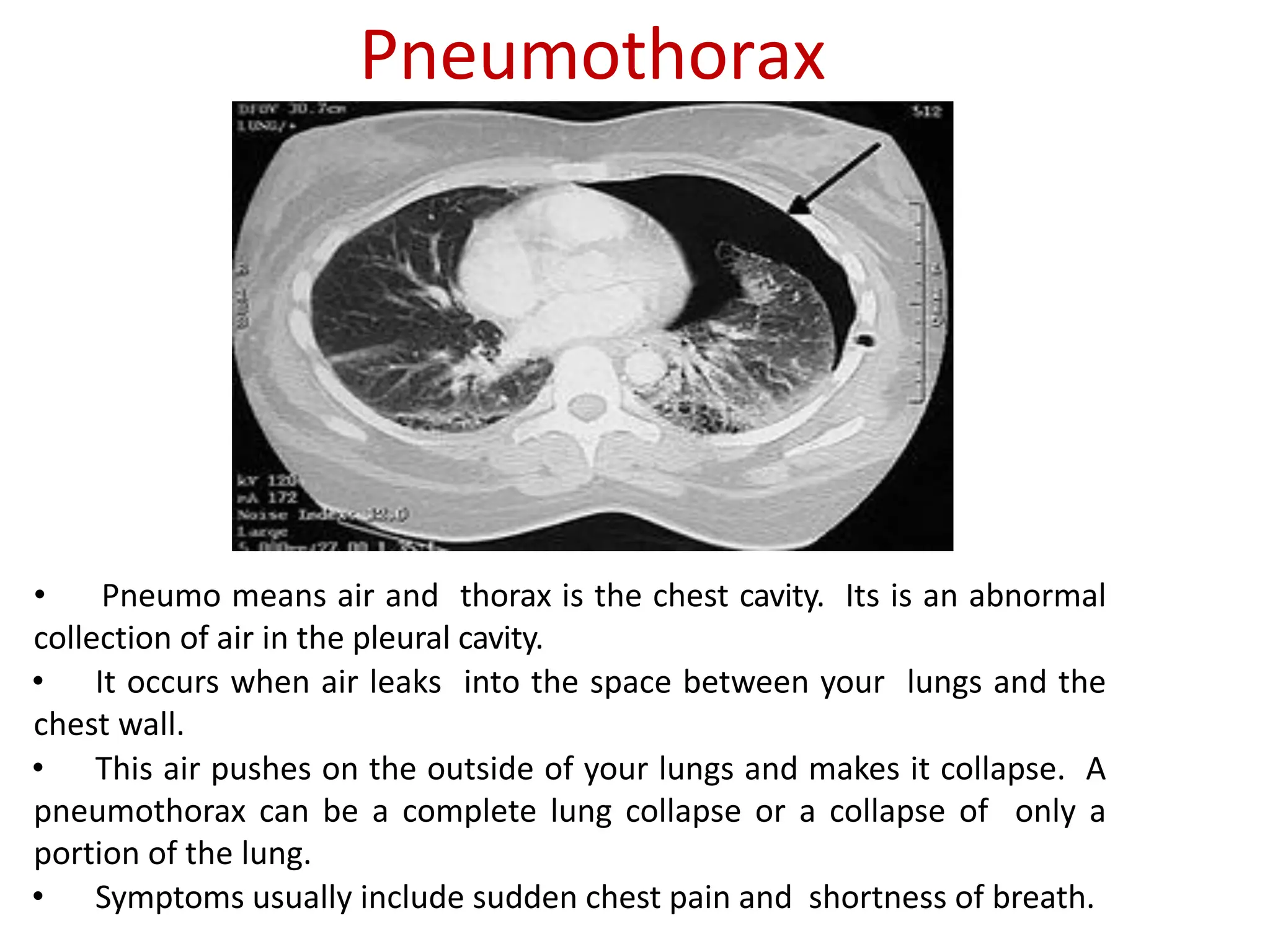
Pneumothorax
• Pneumo meansair and thorax is the chest cavity. Its is an abnormal
collection of air in the pleural cavity.
• It occurs when air leaks into the space between your lungs and the
chest wall.
• This air pushes on the outside of your lungs and makes it collapse. A
pneumothorax can be a complete lung collapse or a collapse of only a
portion of the lung.
• Symptoms usually include sudden chest pain and shortness of breath.
13.
Pulmonary ventilation
The processof gas exchange in the body, called respiration, has three basic
steps:
1. Pulmonary ventilation ( pulmon- lung), or breathing, is the inhalation
(inflow) and exhalation (outflow) of air and involves the exchange of air
between the atmosphere and the alveoli of the lungs.
2. External (pulmonary) respiration is the exchange of gases between the
alveoli of the lungs and the blood in pulmonary capillaries across the
respiratory membrane. In this process, pulmonary capillary blood gains
O2 and loses CO2.
3. Internal (tissue) respiration is the exchange of gases between blood in
systemic capillaries and tissue cells. In this step the blood loses O2 and
gains CO2. Within cells, the metabolic reactions that consume O2 and
give off CO2 during the production of ATP are termed cellular respiration
14.
Factors Affecting PulmonaryVentilation
Lung compliance
• Ability of the lungs to be expanded, stretched, or inflated.
• Depends on Elasticity of the lung tissue refers to the ability of the lung to
inflate easily.
Surface Tension
• The force of attraction between liquid molecules.
• Surfactant reduces the surface tension in the alveoli allowing them to easily
expand to twice their size with each breath and it interferes with the
attraction between fluid molecules.
15.
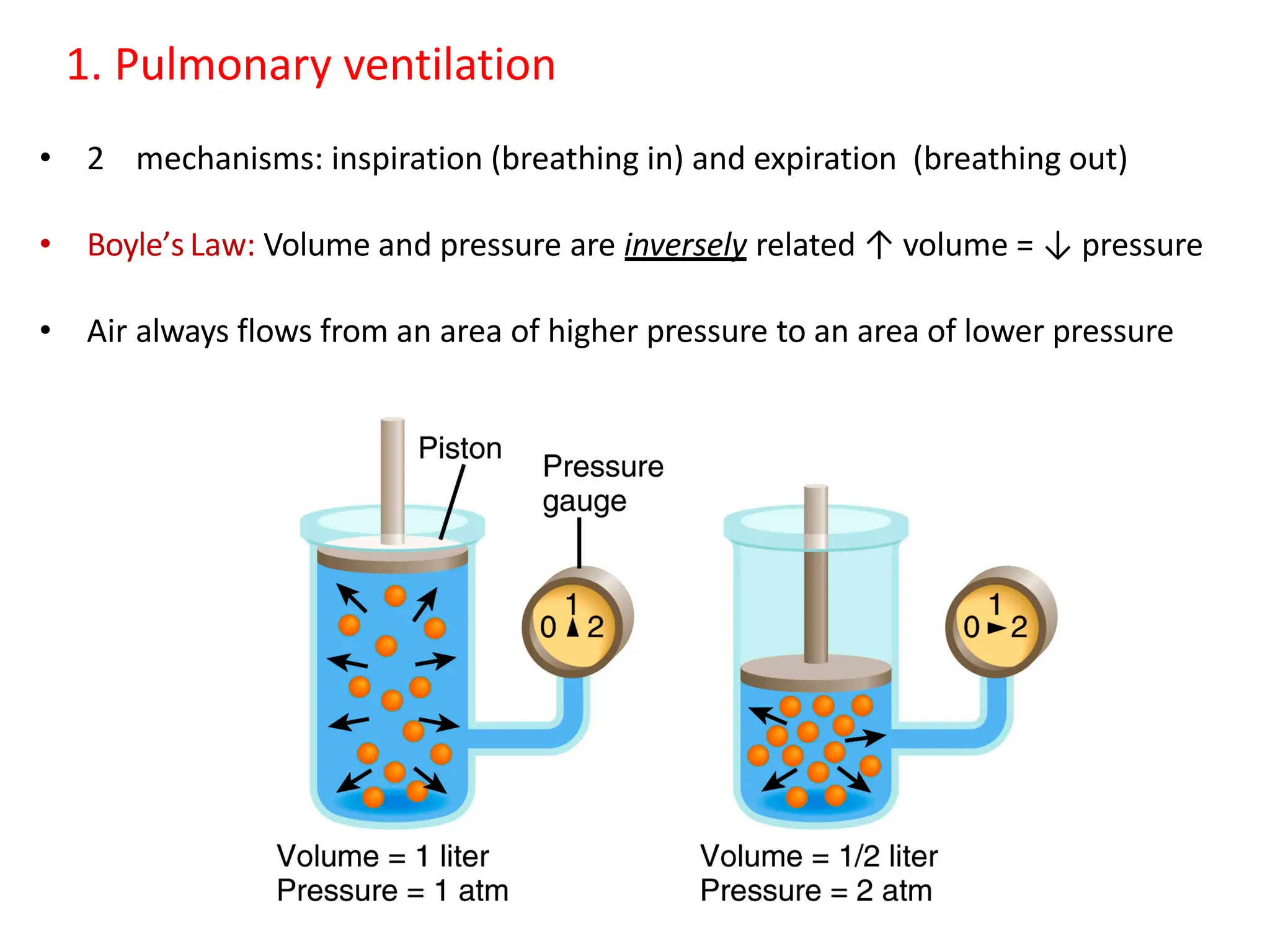
1. Pulmonary ventilation
•2 mechanisms: inspiration (breathing in) and expiration (breathing out)
• Boyle’s Law: Volume and pressure are inversely related ↑ volume = ↓ pressure
• Air always flows from an area of higher pressure to an area of lower pressure
16.
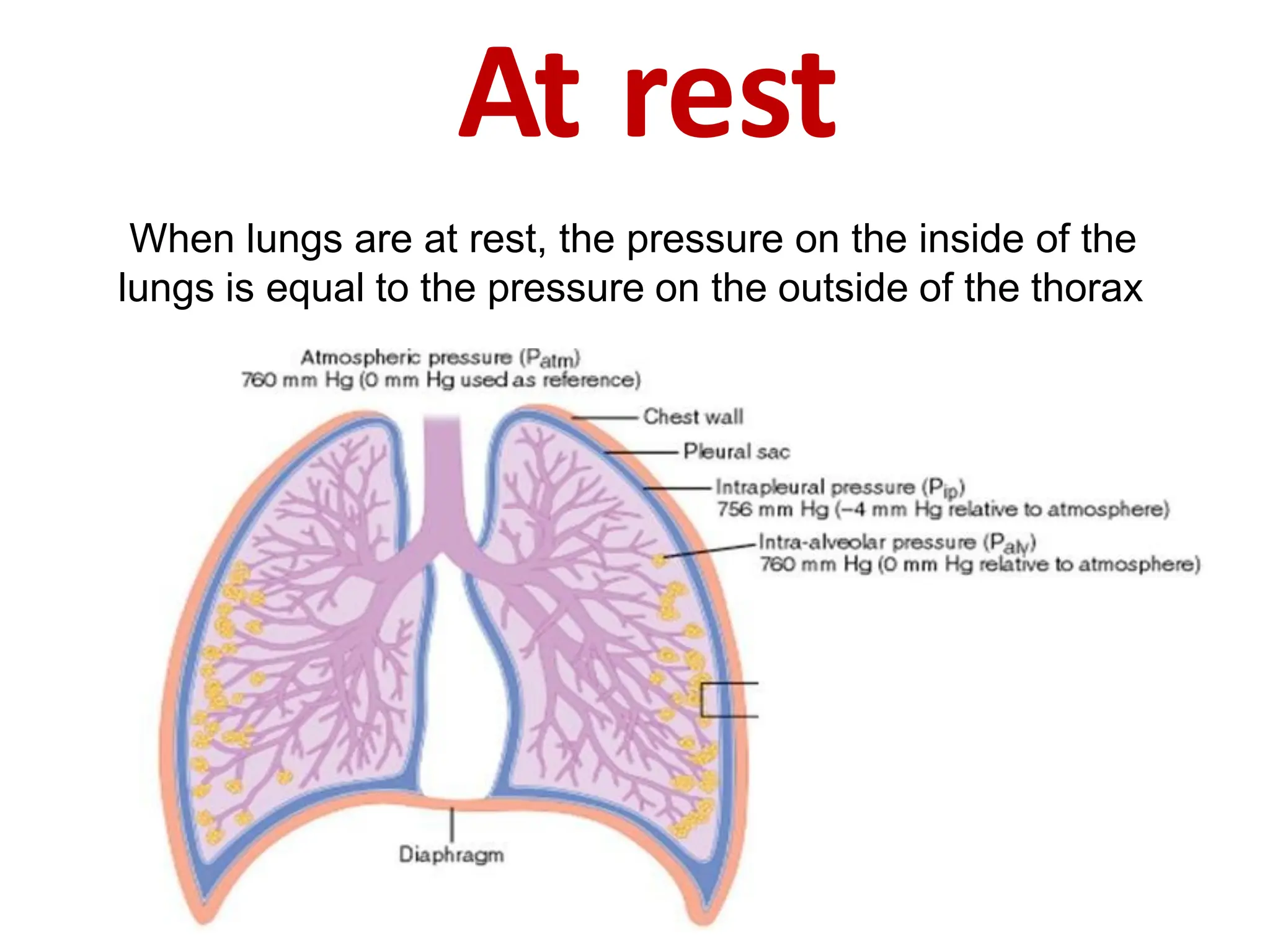
Pulmonary Pressures
Pressure gradient:The difference between intrapulmonary and atmospheric
pressures
• Atmospheric pressure: The pressure exerted by the weight of
the air in atmosphere (~ 760 mmHg at sea level)
• Intra-alveolar (Intrapulmonary) pressure: The pressure inside the lungs
• Intrapleural pressure: The pressure inside the pleural space.
• Transpulmonary pressure The difference betweenthe intra-
alveolar and intrapleural pressures.
17.
Exhalation
Exhalation results fromelastic recoil of the
chest wall and lungs, both of which have a
natural tendency to spring back after they
have been stretched.
Exhalation starts when the inspiratory
muscles relax. As the diaphragm relaxes, its
dome moves superiorly owing to its
elasticity. As the external intercostals relax,
the ribs are depressed.
These movements decrease the vertical,
lateral, and anteroposterior diameters of
the thoracic cavity, which decreases lung
volume.
In turn, the alveolar pressure increases to
about 762 mmHg. Air then flows from the
area of higher pressure in the alveoli to the
area of lower pressure in the atmosphere
20.
Airway resistance
• Theflow of air through the airways depends on both the
pressure difference and the resistance
• Airway resistance is most affected by changes in the diameter
of the bronchioles
– ↓ diameter of the bronchioles = ↑ airway resistance
• During inspiration, the resistance to airflow decreases
• During expiration, the resistance to airflow increases
21.
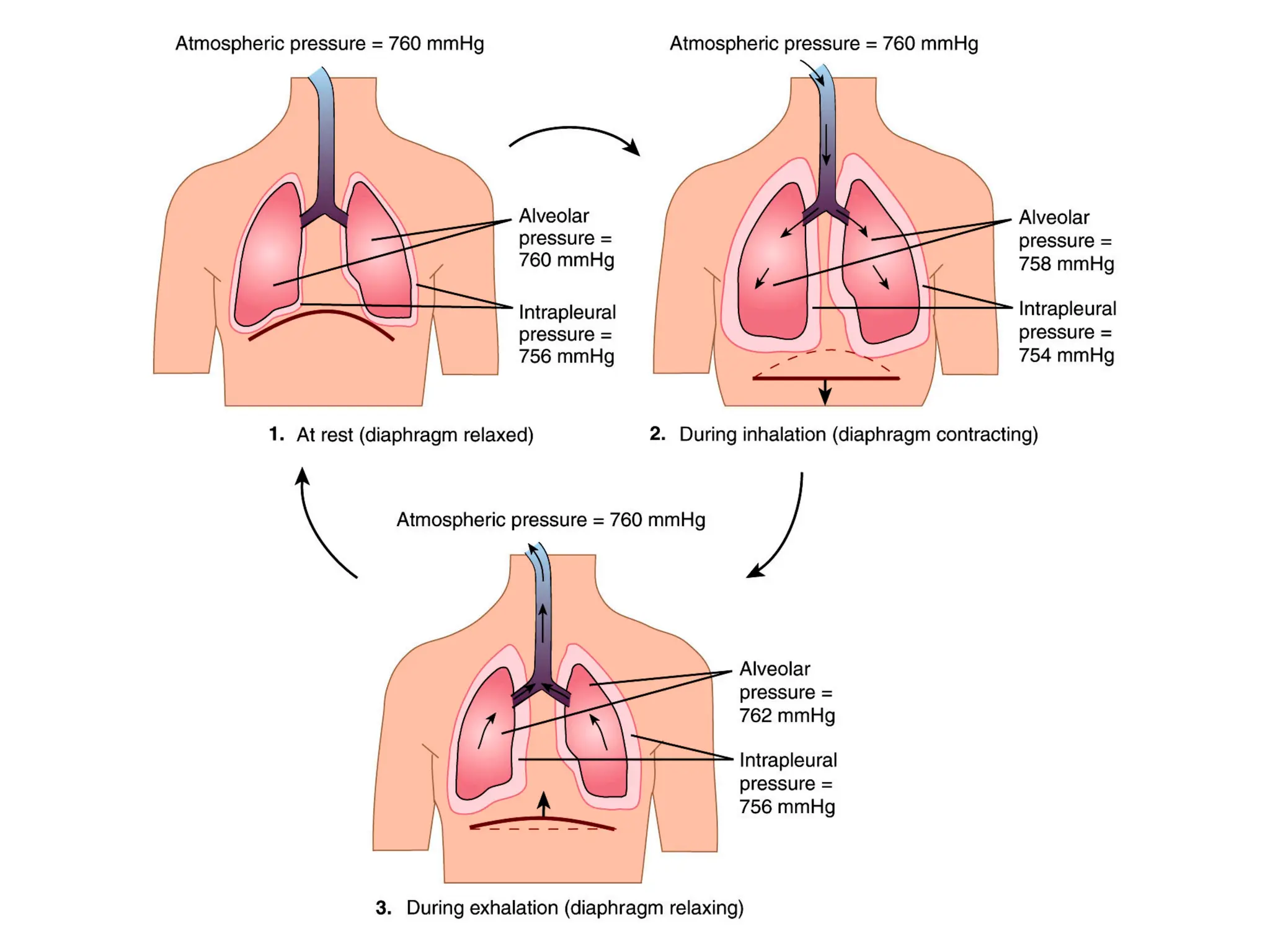
At rest
When lungsare at rest, the pressure on the inside of the
lungs is equal to the pressure on the outside of the thorax
22.
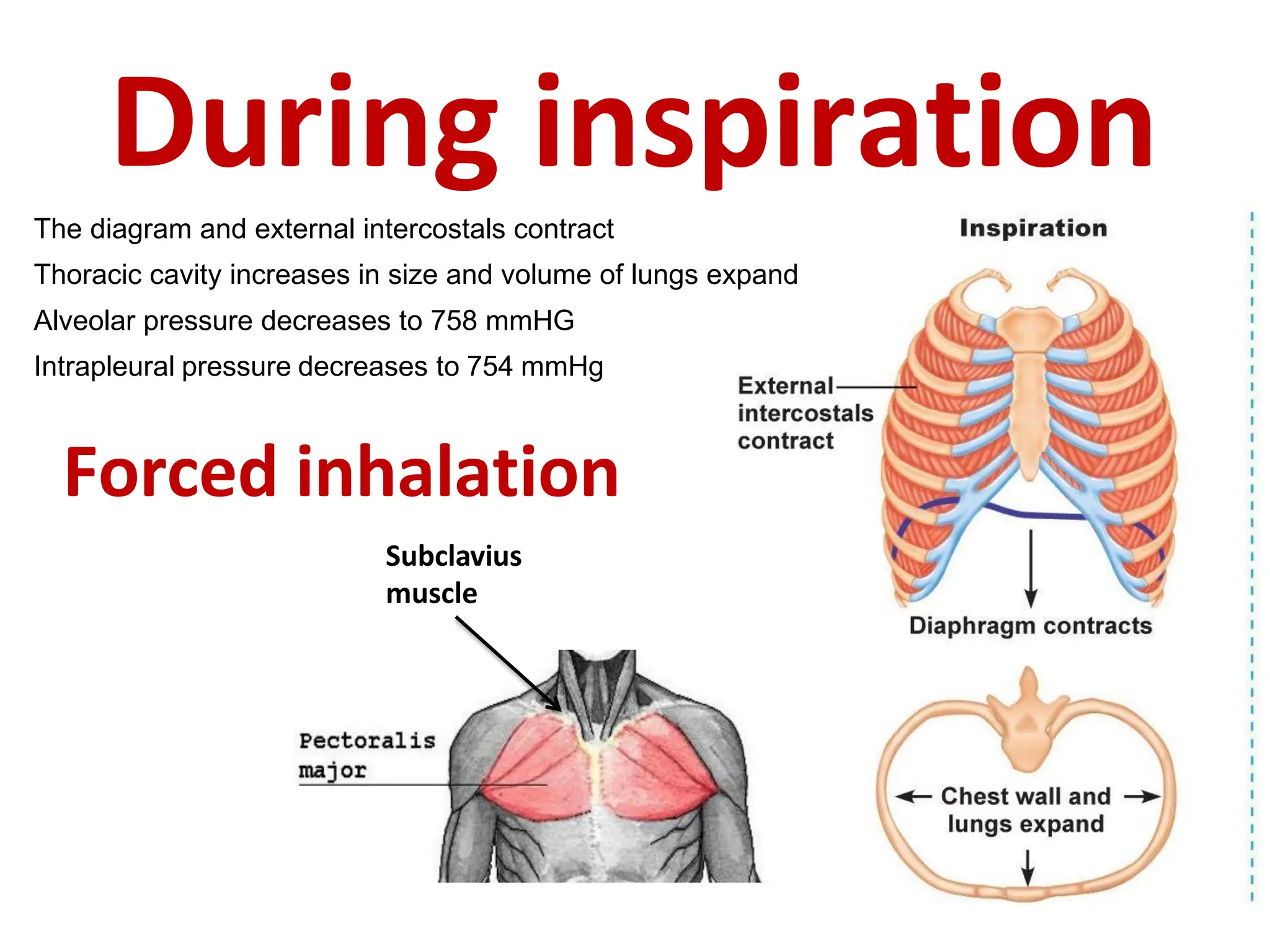
During inspiration
The diagramand external intercostals contract
Thoracic cavity increases in size and volume of lungs expand
Alveolar pressure decreases to 758 mmHG
Intrapleural pressure decreases to 754 mmHg
Subclavius
muscle
Forced inhalation
23.
During exhalation
The diaphragmand external intercostals relax
Thoracic cavity decreases in size and lungs recoil
Alveor pressure increases to 762 mmHg
Intrapleural pressure increases to 756 mmHg
Forced exhalation
24.
Spirometry
The apparatus usedto measure the volume of air exchanged during
breathing is a spirometer or respirometer; the record is called
spirogram
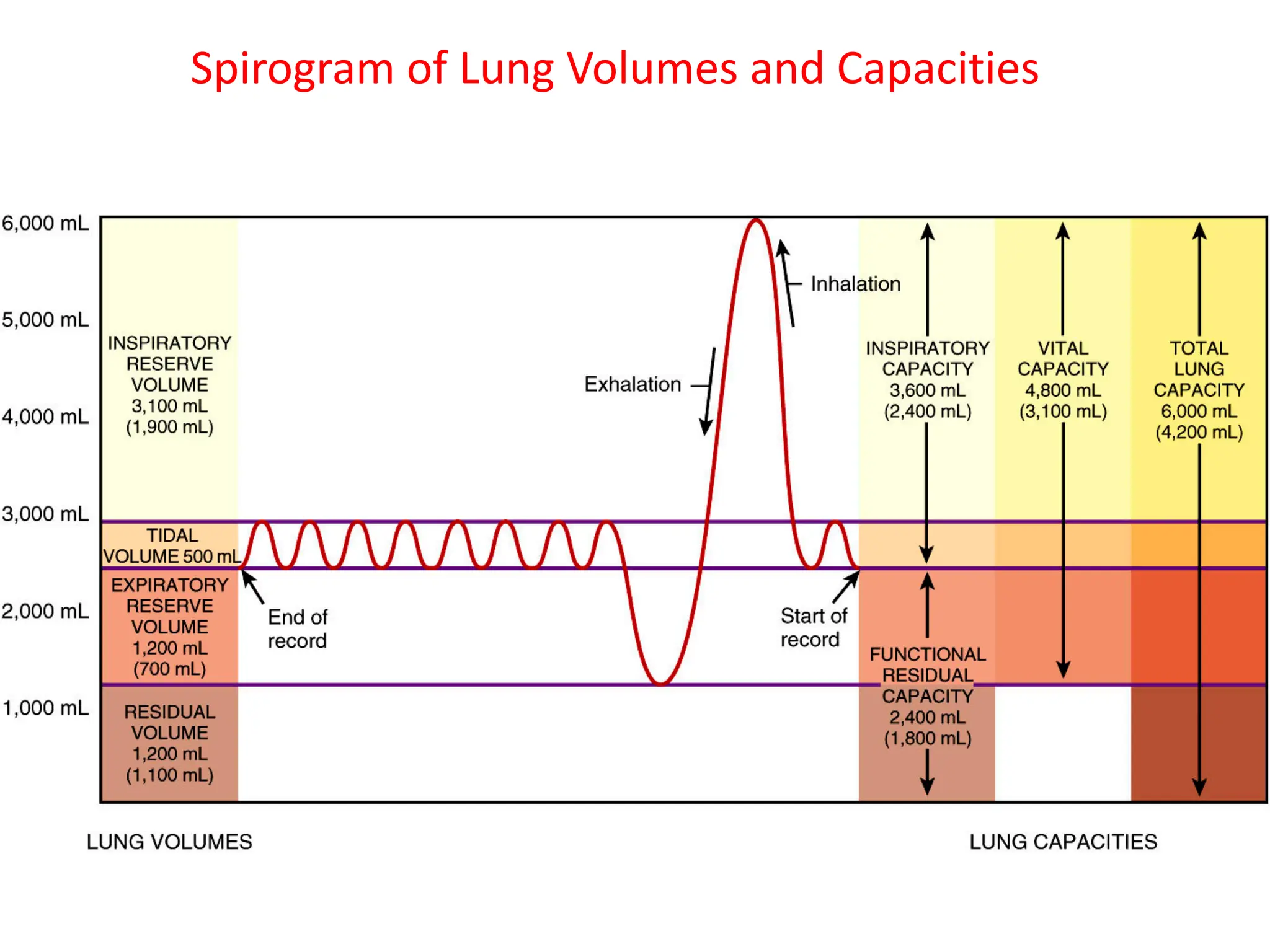
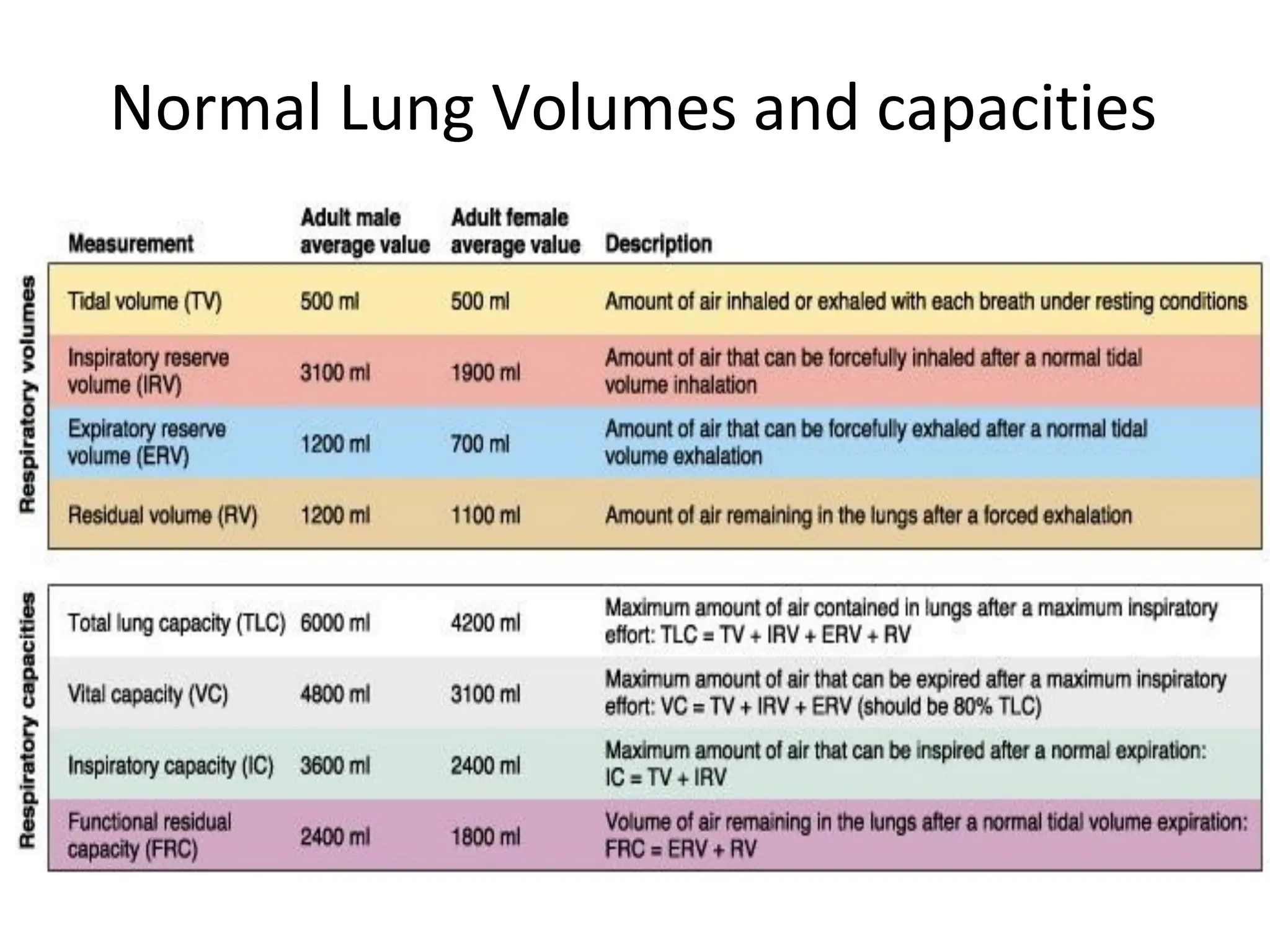
Lung Volumes
• TidalVolume (VT)
– amount of air entering/leaving
lungs in a single, “normal” breath
– 500 ml at rest
• Inspiratory Reserve Volume (IRV)
– additional volume of air that can
be maximally inspired beyond
VT by forced inspiration
– 3100 ml. at rest
• Expiratory Reserve Volume (ERV)
– additional volume of air that can
be maximally expired beyond VT
by forced expiration
– 1200 ml. at rest
28.
• Residual Volume(RV)
– volume of air that
remain in the lungs
after a forced
maximum expiration,
keeping the lungs
partially inflated
– 1200 ml. at rest
Lung Volumes
29.
Lung Capacities
Minute ventilation(MV) = total volume of air inhaled and exhaled each minute
Normal healthy adult averages 12 breaths per minute
moving about 500 ml of air in and out of lungs (tidal volume)
MV = 12 breaths/min x 500 ml/ breath
= 6 liters/ min
Lung capacities are combinations of specific lung volumes.
Total Lung Capacity = Inspiratory Reserve Volume (IRV) + Tidal Volume (TV) + Expiratory
Reserve Volume (ERV) + Residual Volume (RV)= 4800 mL +1200 mL = 6000 mL in males
and 3100 mL+ 1100 mL = 4200 mL in females .
Vital Capacity = Inspiratory Reserve Volume (IRV) + Tidal Volume (TV) + Expiratory Reserve
Volume (ERV)= 4800 mL in males and 3100 mL in females.
Inspiratory Capacity = Inspiratory Reserve Volume (IRV) + Tidal Volume (TV)= 500 mL +
3100 mL = 3600 mL in males and 500 mL +1900 mL =2400 mL in females
Functional Residual Capacity = Expiratory Reserve Volume (ERV) + Residual Volume (RV)=
1200 mL + 1200 mL = 2400 mL in males and 1100 mL + 700 mL = 1800 mL in females
Minute ventilation
The totalvolume of air inspired and expired each minute
minute ventilation (ml/min)
=
tidal volume (L/breath)
0.5 L/ breath x
x respiratory rate (breaths/min)
15 cycles/min
7.5 L/min
32.
Anatomic dead space
•In any average adult, about 70 % of the tidal volume actually
reaches the respiratory portion of the respiratory system,
while 30% remains in air spaces of the conducting portion of
the respiratory system. These areas are known as the
anatomic dead space (VD) that does not undergo respiratory
exchange
• Role: Warms and filtered the air
33.
Alveolar ventilation rate
Todetermine how much fresh air enters the alveoli per minute;
Alveolar ventilation rate (ml/min)
=
(tidal volume – anatomic dead space) x respiratory rate
5250 ml/min
Tidal volume and anatomic dead space: (ml/breath)
Respiratory rate: (breaths/min)
34.
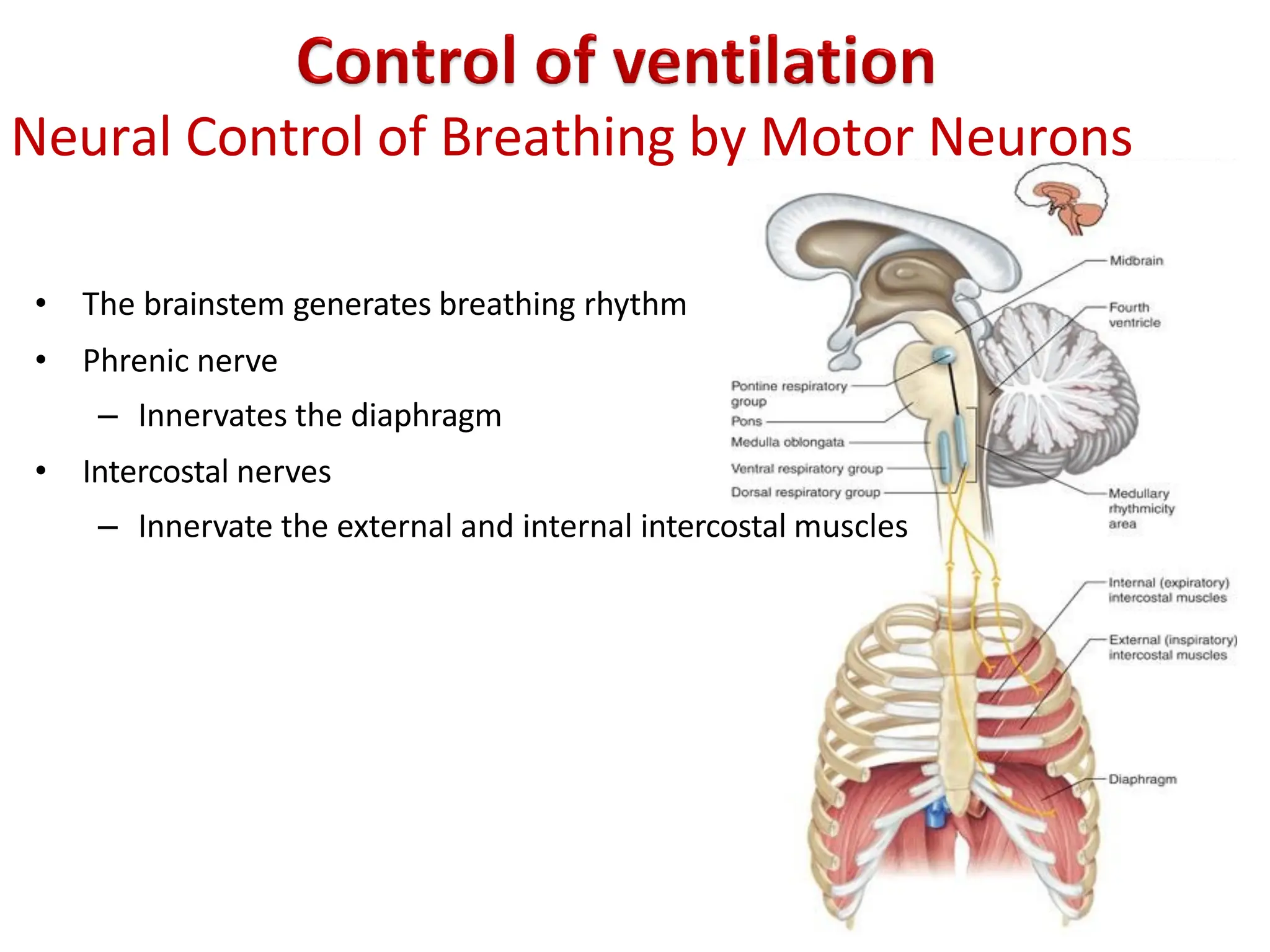
Neural Control ofBreathing by Motor Neurons
• The brainstem generates breathing rhythm
• Phrenic nerve
– Innervates the diaphragm
• Intercostal nerves
– Innervate the external and internal intercostal muscles
35.
Generation of theBreathing Rhythm by the
Brainstem
• Central control of respiration is not completely
understood
• Research indicates that respiratory control centers
are located in the brainstem
• Respiratory control centers include…
– Medullary Rhythmicity Area of the medulla oblongata
– Pneumotaxic Area of the pons
– Apneustic Center of the pons
36.
Medullary Rhythmicity Area
•Includes two groups of
neurons:
– Dorsal Respiratory Group
– Ventral Respiratory Group
37.
Medullary Rhythmicity Area
TheDorsal Respiratory Group
• The medullary inspiratory center
• Functions in quiet breathing
– The respiratory cycle is repeated 12 - 15 times/minute
• Quiet breathing - Inhalation
– The dorsal inspiratory neurons transmit nerve impulses via the phrenic
and intercostal nerves to the diaphragm and external intercostal
muscles
– When these muscles contract, the lungs fill with air
38.
Medullary Rhythmicity Area
TheVentral Respiratory Group
• Inspiration and expiration center
• Functions only in forced breathing
• The ventral expiratory neurons transmit nerve impulses
to the muscles of breathing
– Accessory inspiratory muscles
– The internal intercostals
– The abdominal muscles
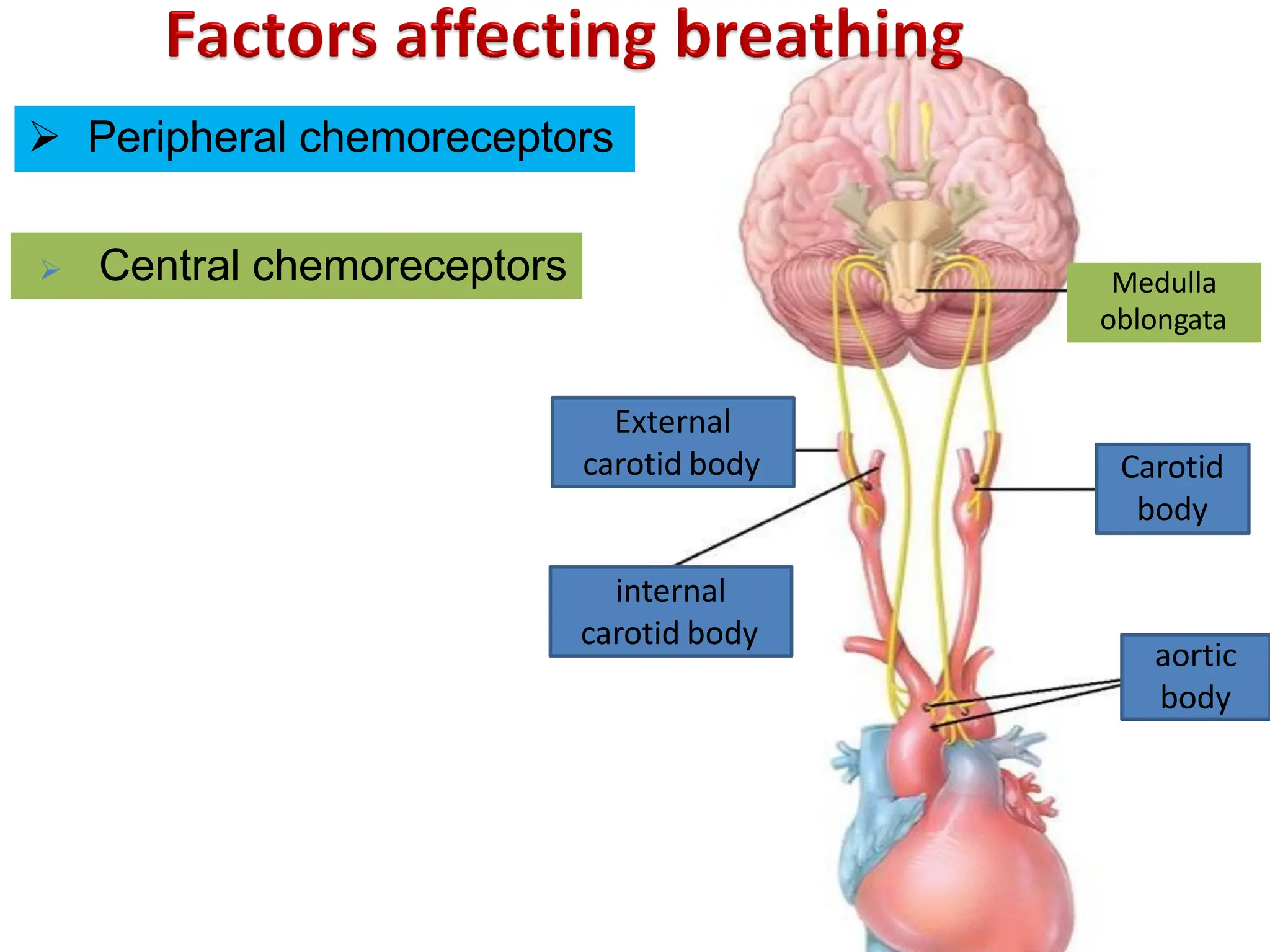
Peripheral Chemoreceptors
• Location:
–Carotid and aortic bodies
– Connected to medulla by afferent neurons in the glossopharyngeal (N IX)
nerve and vagus ( N X) nerve
• Chemical concentration of the blood is most important
– Changing levels of O2,CO2 and pH of the blood
– Sensitive to low arterial O2 concentrations (below 60 mmHg)
43.
Central Chemoreceptors
• Locatedin the ventro-lateral surface of the medulla
• sensitive to a increase of [CO2] and H+ ion concentration
in arterial blood and CSF
• Increased CO2 = increased concentration of H+ ions (↓
pH)
• ↓ arterial pH causes the respiratory system to attempt to
restore normal blood pH by…
– ↑ ventilation to decrease CO2 levels
– This results in an increase in pH to normal levels
44.
Disturbances in Respiration
Hypercapnea
•An ↑ in the arterial CO2 concentration with a resultant ↓ in
pH
• This condition stimulates the…
– Central chemoreceptors and peripheral chemoreceptors
– Medullary respiratory centers
• Stimulates an increase in ventilation
Transport of oxygenand carbon
dioxide
• Blood transports gases between the lungs and body tissue
1) Oxygen transport
2) Carbon dioxide transport
47.
Oxygen transport
• Dissolvedin watery blood plasma (2%)
• In chemical combination with hemoglobin inside red blood
cells (98%) to form the oxyhemoglobin (HbO2) in a reversible
reaction
Carbon dioxide transport
ØDissolved in the blood plasma (7%)
Ø In chemical combination with
carbaminohemoglobin (23%)
hemoglobin as
Ø Transported in plasma as bicarbonate ions (HCO3-) (70%)



























![Central Chemoreceptors
• Located in the ventro-lateral surface of the medulla
• sensitive to a increase of [CO2] and H+ ion concentration
in arterial blood and CSF
• Increased CO2 = increased concentration of H+ ions (↓
pH)
• ↓ arterial pH causes the respiratory system to attempt to
restore normal blood pH by…
– ↑ ventilation to decrease CO2 levels
– This results in an increase in pH to normal levels](https://image.slidesharecdn.com/therespiratorysystem250410111254-250603041938-31bcfd7c/75/The-Respiratory-system-_250410_111254-pdf-43-2048.jpg)