
More Related Content
What's hot
What's hot (20)
Similar to Respiratory system 1
Similar to Respiratory system 1 (20)
More from Cindrella Zinnia Burge
More from Cindrella Zinnia Burge (16)
Recently uploaded
Recently uploaded (20)
Respiratory system 1
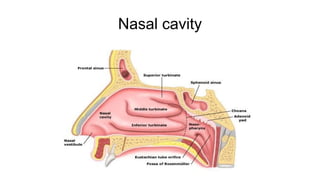
- 1. Nasal cavity
- 2. Epiglottis
- 4. Larynx
- 8. Trache a
- 15. Asthma • Asthma is a chronic inflammatory disease of the airways that causes airway hyper-responsiveness, mucosal edema, and mucus production
- 16. INCIDENCE • common chronic disease of childhood • For most patients, asthma is a disruptive disease, affecting school and work attendance, occupational choices, physical activity, and general quality of life.
- 19. • Air pollutants, cold, heat, weather changes, strong odors or perfumes, smoke), exercise, stress or emotional upset, medications, viral respiratory tract infections, and gastroesophageal reflux
- 27. Clinical manifestations • 3 most common symptoms of asthma are cough, dyspnea, and wheezing. • An asthma attack often occurs at night or early in the morning, possibly because of circadian variations • Sometimes mucus is so tightly obstructed patients cannot even cough it up. • Chest tightness • Expiration requires effort and becomes prolonged
- 28. • diaphoresis • Tachycardia • hypoxemia and central cyanosis
- 32. Diagnostic findings • History collection • Physical examination • Sputum and blood tests may disclose eosinophilia • Arterial blood gas analysis and pulse oximetry reveal hypoxemia
- 33. Prevention • Identify the substances that precipitate the symptoms. • Possible causes are dust, dust mites, cockroaches, certain types of cloth, pets, horses, detergents, soaps, certain foods, molds, and pollens. • Avoid the causative agents whenever possible. Knowledge is the key to quality asthma care.
- 34. Complications • Status asthmaticus • Respiratory failure, • Pneumonia, and atelectasis. • Airway obstruction, results in hypoxemia • Frequently dehydrated from diaphoresis and insensible fluid loss with hyperventilation.
- 35. Medical mangement Pharmacologic Therapy 1. Quick-Relief Medication Short-acting beta2-adrenergic agonists (albuterol levalbuterol Anticholinergics (eg, ipratropium bromide) 2. Long-Acting Control Medications » Corticosteroids - Inhaled Corticosteroids (ICs) eg:beclomethasone dipropionate - Systemic corticosteroids eg: methylprednisolone
- 36. Nursing Management • Obtains a history of allergic reactions to medications before administering medications • Identifies medications the patient is currently taking • Administers medications as prescribed and monitors the patient’s responses to those medications. • Administers fluids if the patient is dehydrated
- 37. Lung Abscess • Necrosis of the pulmonary parenchyma caused by microbial infection • Lung abscess, the chest x-ray demonstrates a cavity of at least 2 cm.
- 39. Etiology • aspiration of foreign material • Impaired cough reflexes who cannot close the glottis • Swallowing difficulties. • central nervous system disorders (eg, seizure, stroke) • Drug addiction, alcoholism, esophageal disease, or compromised immune function • Patients without teeth and those receiving nasogastric tube feedings • altered state of consciousness due to anesthesia.
- 41. Chronic Obstructive Pulmonary Disease (COPD) • A preventable and treatable disease • Characterized by airflow limitation that is not fully reversible, progressive and an abnormal inflammatory response of the lung to harmful particles or gases”
- 42. • COPD may include diseases that cause airflow obstruction (eg, emphysema, chronic bronchitis)
- 43. Chronic Bronchitis • Defined as the presence of cough and sputum production for at least 3 months in each of 2 consecutive years. • In many cases, smoke or other environmental pollutants irritate the airways, resulting in inflammation and hypersecretion of mucus.
- 44. Mucus plugging of the airway reduces ciliary function. Bronchial walls also become thickened, further narrowing the bronchial lumen
- 45. • Alveoli adjacent to the bronchioles may become damaged and fibrosed, resulting in altered function of the alveolar macrophages. • The patient becomes more susceptible to respiratory infection
- 46. Emphysema • In emphysema, impaired oxygen and carbon dioxide exchange results from destruction of the walls of overdistended alveoli
- 47. Emphysema • Destruction of the walls of the alveoli • No proper gaseous exchange • Results in hypercapnia( CO2 ) and hypoxaemia
- 49. Clinical Manifestations • chronic cough, sputum production, and dyspnea • Weight loss • development of airflow limitation • Patients with COPD are at risk for respiratory insufficiency and respiratory infections
- 50. • Typical posture of a person with chronic obstructive pulmonary disease (COPD)— primarily emphysema. The person tends to lean forward and uses the accessory muscles of respiration to breathe, forcing the shoulder girdle upward and causing the supraclavicular fossae to
- 52. Assessment and Diagnostic Findings • Pulmonary function test • Spirometry • Arterial blood gas measurements • chest x-ray • computed tomography (CT)
- 53. Complications • Respiratory insufficiency and failure are major life threatening complications of COPD • pneumonia, chronic atelectasis, pneumothorax, and pulmonary arterial hypertension (cor pulmonale).
- 54. Medical Management Pharmacologic Therapy Bronchodilators – dilate the bronchi and bronchioes – given through Inhaler
- 58. • Oxygen Therapy Surgical Management Bullectomy Lung Transplantation
- 59. Empyema An empyema is an accumulation of thick, purulent fluid within the pleural space, often with fibrin development and a loculated (walled-off) area where infection is located
- 61. Etiology • As a complication of bacterial pneumonia or lung abscess • Penetrating chest trauma • Hematogenous infection of the pleural space • Nonbacterial infections, and iatrogenic causes (after thoracic surgery or thoracentesis)
- 62. Pathophysiology • Due to etiological factors • At first the pleural fluid is thin, with a low leukocyte count, Fibropurulent stage • it encloses the lung within a thick exudative membrane
- 63. Clinical Manifestations • fever, • night sweats, • pleural pain, • cough, dyspnea, • anorexia, weight loss.
- 64. Assessment and Diagnostic Findings • Chest auscultation demonstrates decreased or absent breath sounds over the affected area, and there is dullness on chest percussion as well as decreased fremitus. • Chest CT. • Diagnostic thoracentesis is performed, often under ultrasound guidance.
- 65. Medical Management • To drain the pleural cavity and to achieve complete expansion of the lung. • The fluid is drained, and appropriate antibiotics, in large doses, are prescribed based on the causative organism. • Sterilization of the empyema cavity requires 4 to 6 weeks of antibiotics. • Drainage of the pleural fluid depends on the stage of the disease and is accomplished by one of the following methods:
- 66. • Needle aspiration (thoracentesis) with a thin percutaneous catheter, if the volume is small and the fluid is not too purulent or too thick
- 67. • Tube thoracostomy (chest drainage using a large diameter intercostal tube attached to water-seal drainage with fibrinolytic agents instilled through the chest tube
- 69. • Open chest drainage via thoracotomy, including potential rib resection, to remove the thickened pleura, pus, and debris and to remove the underlying diseased pulmonary tissue
- 70. • The pleural space is monitored by serial chest x- rays, and the patient should be informed that treatment may be long term.
- 71. Nursing Management • Instruct the patient in lung-expanding breathing exercises • Provides care specific to the method of drainage of the pleural fluid (eg, needle aspiration, closed chest drainage, rib resection and drainage). • When the patient is discharged home, the nurse instructs the patient and family on care of the drainage system and drain site, measurement and observation of drainage, signs and symptoms of infection, and how and when to contact the health
- 73. Pleural Effusion • Pleural effusion, a collection of fluid in the pleural space, is rarely a primary disease process; it is usually secondary to other diseases. • Normally, the pleural space contains a small amount of fluid (5 to 15 mL), which acts as a lubricant that allows the pleural surfaces to move without friction
- 75. Etiology • As a complication of heart failure • TB • Pneumonia • Pulmonary infections (particularly viral infections) • Nephrotic syndrome • Connective tissue disease, pulmonary embolus, and neoplastic tumors.
- 76. Clinical Manifestations • Fever • Chills • Pleuritic chest pain • Dyspnea, difficulty lying flat, and coughing. • The severity of symptoms is determined by the size of the effusion, the speed of its formation, and the underlying lung disease. (large pleural effusion causes dyspnea (shortness of breath) and small to moderate pleural effusion causes minimal or no dyspnea.
- 78. • Decreased or absent breath sounds, decreased fremitus, and • A dull, flat sound on percussion. • Tracheal deviation away from the affected side may also be apparent. • Physical examination, chest x-ray, chest CT, and thoracentesis confirm the presence of fluid. • Pleural fluid is analyzed by bacterial culture, Gram stain, acid-fast bacillus stain (for TB), red and white blood cell counts, chemistry studies (glucose, amylase, lactate dehydrogenase, protein), cytologic analysis for malignant Diagnostic findings
- 79. Medical Management • Treat the cause of the pleural effusion; to prevent reaccumulation of fluid • Thoracentesis • chemical pleurodesis – With the chest tube approach, after the agent (eg, talc or another chemical irritant) is instilled, the chest tube is clamped for 60 to 90 minutes and the patient is assisted to assume various positions to promote uniform distribution of the agent
- 80. • Surgical pleurectomy • Implantation of a pleuroperitoneal shunt.
- 81. Nursing Management • Implementing the medical regimen. • The nurse prepares and positions the patient for thoracentesis and offers support throughout the procedure. • The nurse is responsible for making sure the thoracentesis fluid amount is recorded and sent for appropriate laboratory testing. • If a chest tube is inserted for talc instillation, pain management is a priority and the nurse helps the patient assume positions that are the least painful. • The nurse evaluates the patient’s pain level and administers analgesic agents as prescribed and as needed.
- 82. Pneumonia • Pneumonia is an inflammation of the lung parenchyma caused by bacteria (mycobacteria), fungi, and viruses.
- 83. Incidence • Common causes of death from infectious diseases in the United States • Together they account for nearly 60,000 deaths annually and rank as the eighth leading cause of death in the United States
- 84. Etiology
- 85. Pathophysiology
- 86. • Pneumonia affects both ventilation and diffusion. An inflammatory • reaction can occur in the alveoli, producing an • exudate that interferes with the diffusion of oxygen and carbon • dioxide. White blood cells, mostly neutrophils, also migrate • into the alveoli and fill the normally air-filled spaces. • Areas of the lung are not adequately ventilated because of • secretions and mucosal edema that cause partial occlusion • of the bronchi or alveoli, with a resultant decrease in alveolar • oxygen tension. Bronchospasm may also occur in patients • with reactive airway disease. Because of hypoventilation, a • ventilation–perfusion mismatch occurs in the affected area • of the lung. Venous blood entering the pulmonary circulation • passes through the underventilated area and travels to • the left side of the heart poorly oxygenated. The mixing of • oxygenated and unoxygenated or poorly oxygenated blood • eventually results in arterial hypoxemia.
- 87. • If a substantial portion of one or more lobes is involved, • the disease is referred to as lobar pneumonia. The term bronchopneumonia • is used to describe pneumonia that is distributed • in a patchy fashion, having originated in one or more • localized areas within the bronchi and extending to the adjacent • surrounding lung parenchyma. Bronchopneumonia
- 88. Risk Factors • Travel or exposure to certain environments and residence in a long-term care facility. • Less immunity against infections • Heart failure, diabetes, alcoholism, COPD, and AIDS
- 89. Clinical Manifestations • Sudden onset of chills • Rapidly rising fever (38.5 to 40.5C [101 to 105F]) • Pleuritic chest pain that is aggravated by deep breathing and coughing. • Tachypnea (25 to 45 breaths/min) • Respiratory distress (eg, shortness of breath, use of accessory muscles in respiration) • The pulse is rapid and bounding, and it usually increases about 10 bpm for every degree (Celsius) of
- 90. • Nasal congestion, Sore throat • Headache • Myalgia • Pharyngitis
- 91. • Mucoid or mucopurulent sputum is expectorated (sometimes blood tinged) • Cheeks are flushed and the lips and • Central cyanosis (a late sign of poor oxygenation [hypoxemia]) • Orthopnea (shortness of breath when reclining) • Poor Appetite • Diaphoretic and tires easily.
- 92. • Crackles indicate consolidation of lung tissue • Percussion dullness, egophony (when auscultated, the spoken “E” becomes a loud, nasal-sounding “A”)
- 95. Assessment and Diagnostic Findings • history • physical examination, • chest x-ray, blood culture • and sputum examination. The sputum sample is obtained by having patients do the following: (1) rinse the mouth with water to minimize contamination by normal oral flora, (2) breathe deeply several times, (3) cough deeply, and (4) expectorate
- 96. • Bronchoscopy is used in patients with acute severe infection
- 97. Prevention • A pneumococcal vaccine provides specific prevention against pneumococcal pneumonia and other infections caused by S. pneumoniae (otitis media, other upper respiratory tract infections). – Vaccination against pneumococcal infection is advised for the following: People 65 years of age or older Immunocompetent people chronic illness (eg, cardiovascular disease, pulmonary disease, diabetes
- 98. Medical Management • Pharmacologic Therapy – Appropriate antibiotics • Trimethoprim/ sulfamethoxazole (TMP-SMZ) (bacterial pneumonia) • Voriconazole , anidulafungin, caspofungin (fungal pneumonia) • Isoniazid plus rifampin plus ethambutol pyrazinamide (TB) • Clindamycin or beta- lactam antibiotics (Pneumonia from Aspiration)
- 99. • Intravenous (IV) to oral therapy when they are hemodynamically stable
- 100. • Ceftriaxone, ampicillin/sulbactam, levofloxacin, or ertapenem • aminoglycoside plus linezolid or vancomycin. • The patient’s status must be assessed 72 hours after the initiation of therapy, and antibiotics should be discontinued or modified based on the culture results
- 101. Complications • Shock and Respiratory Failure • Hypotension and shock and respiratory failure (especially with gram-negative • Heart failure, cardiac dysrhythmias, pericarditis, and myocarditis • Pleural effusion • Lung abscess
- 102. Nursing Diagnoses • Based on the assessment data, the major nursing diagnoses • may include the following: • • Ineffective airway clearance related to copious tracheobronchial • secretions • • Activity intolerance related to impaired respiratory • function • • Risk for deficient fluid volume related to fever and a • rapid respiratory rate • • Imbalanced nutrition: less than body requirements • • Deficient knowledge about the treatment regimen • and preventive health measures
- 103. Atelectasis • Atelectasis refers to closure or collapse of alveoli • lobar, or overall lung volume. • Most common atelectasis is acute, which occurs most often in the postoperative setting or immobilized people and have a shallow, monotonous breathing pattern. • Excess secretions or mucous plugs may also cause obstruction of airflow and result in atelectasis in an area of the lung. • Atelectasis is observed in patients with a chronic airway obstruction that impedes or blocks air flow to an area of the lung (eg, obstructive atelectasis in the patient with
- 104. Pathophysiology result of reduced ventilation or any blockage obstructs passage of air ventilation. lung becomes airless and the alveoli collapses Signs and symptoms of the disease
- 105. Clinical Manifestations • Atelectasis usually is insidious – dyspnea, cough, and sputum production. – tachycardia, tachypnea, pleural pain, and central cyanosis – The chronic nature of the alveolar collapse predisposes patients to infection distal to the obstruction
- 106. Assessment and Diagnostic Findings • hypoxemia. • Decreased breath sounds and crackles are heard • A chest x-ray may suggest a diagnosis, may reveal patchy infiltrates or consolidated areas. • Pulse oximetry (SpO2) may demonstrate a low saturation of hemoglobin with oxygen (less than 90%) or a lower-than-normal partial pressure of arterial oxygen (PaO2).
- 107. Prevention • Frequent turning, early mobilization, and strategies to expand the lungs and to manage secretions. • Voluntary deep-breathing maneuvers (at least every 2 hours) • Patient education and reinforcement are key to the success • The use of incentive spirometry or voluntary deep breathing enhances lung expansion, decreases the potential for airway closure, and may generate a cough. • chest physical therapy (postural drainage and chest
- 108. Management
- 109. Pulmonary Embolism • Pulmonary embolism (PE) refers to the obstruction of the pulmonary artery or one of its branches by a thrombus (or thrombi) that originates somewhere in the venous system or in the right side of the heart. • .
- 111. Etiology • Age older than 50 years • Prolonged immobility
- 112. Heart failure
- 114. Prolonged immobility
- 115. Pathophysiology
Editor's Notes
- In some instances, a lateral decubitus x-ray is obtained. For this x-ray, the patient lies on the affected side in a side-lying position. A pleural effusion can be diagnosed because this position allows for the “layering out” of the fluid, and an air–fluid line is visible.
- A pleuroperitoneal shunt consists of two catheters connected by a pump chamber containing two one-way valves. Fluid moves from the pleural space to the pump chamber and then to the peritoneal cavity. The patient manually pumps on the reservoir daily to move fluid from the pleural space to the peritoneal space.