Downloaded 351 times


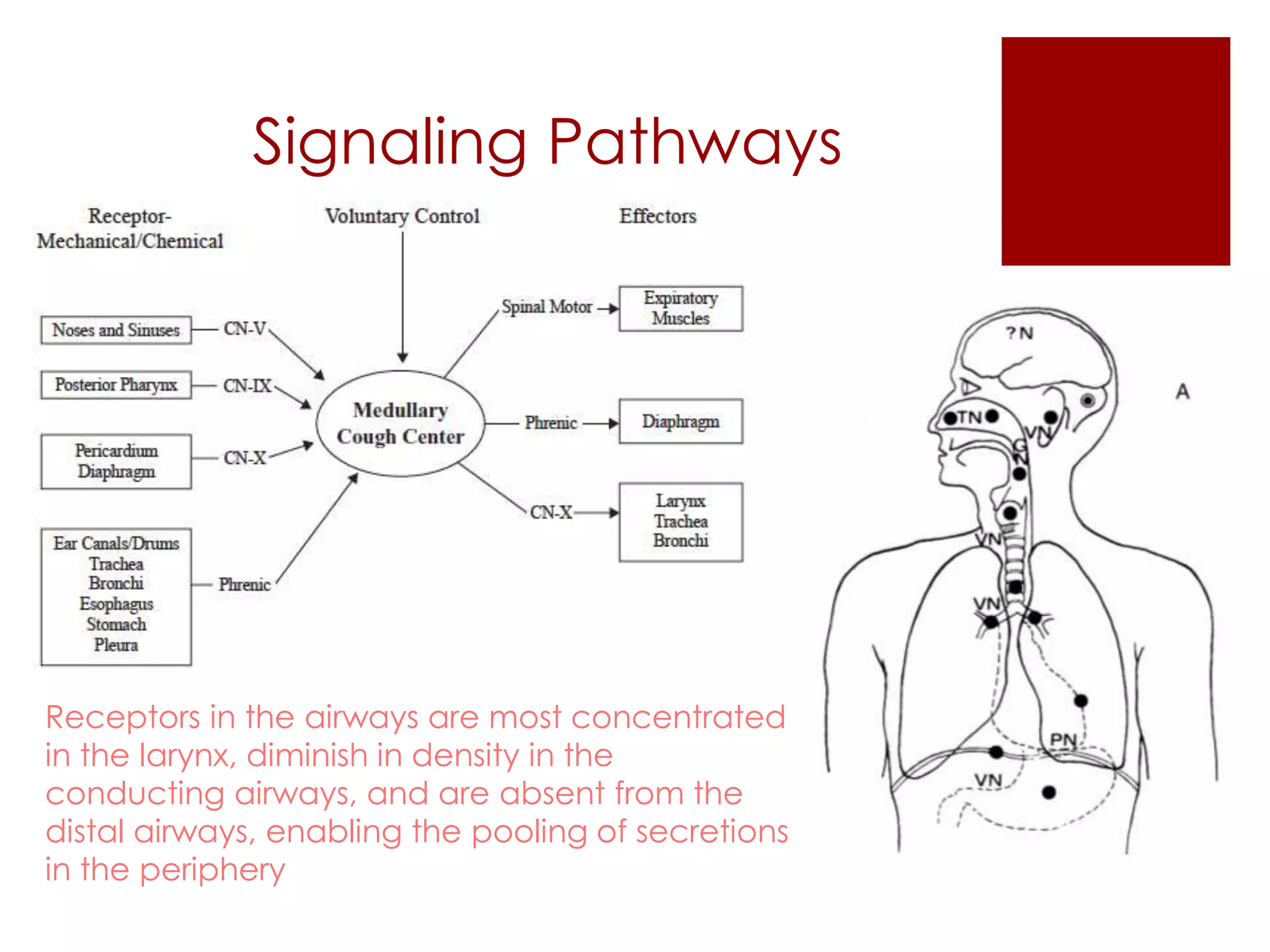






















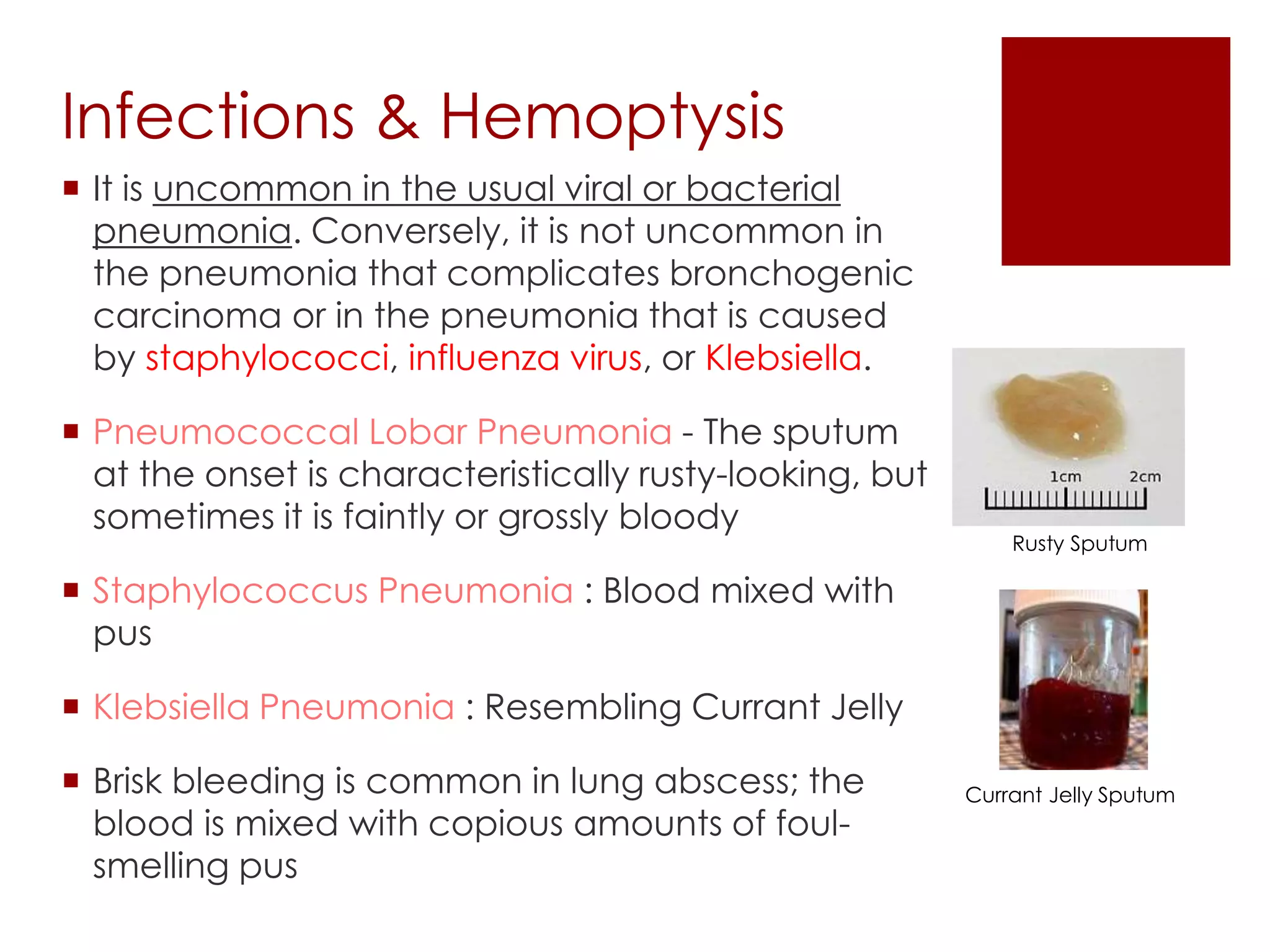






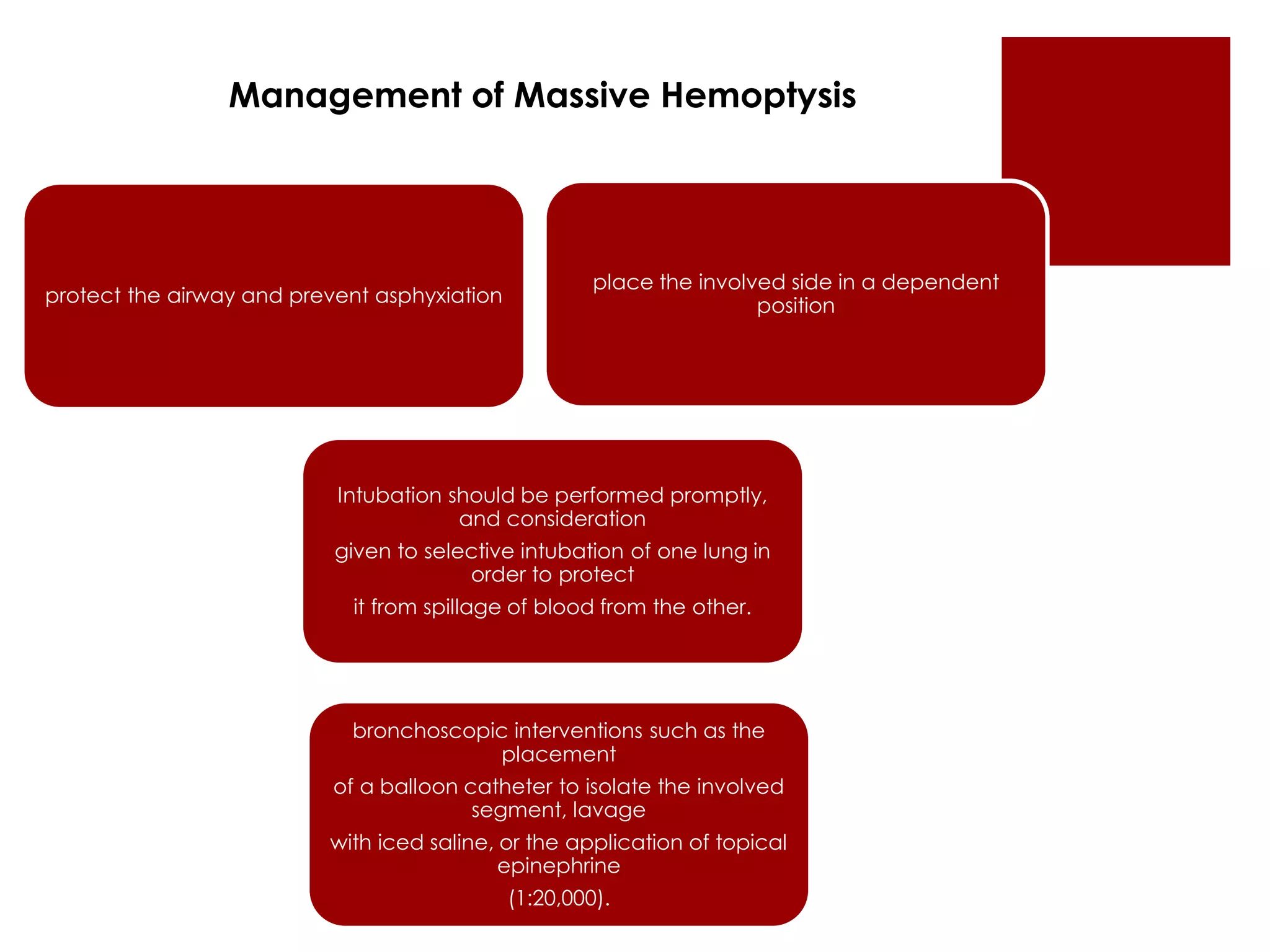


This document defines cough and hemoptysis (coughing up blood) and discusses their causes and characteristics. It provides two definitions of cough from the European Respiratory Society. Cough is initiated by receptors in the airways and involves a rapid inspiration followed by forced expiration and expulsion of air. Hemoptysis can be life-threatening and requires prompt evaluation. Common causes of cough and hemoptysis include infections like pneumonia, conditions like bronchitis or bronchiectasis, and cancers. Medications are discussed that can treat cough through expectorant, anti-tussive, antihistamine, and bronchodilator actions.























































































