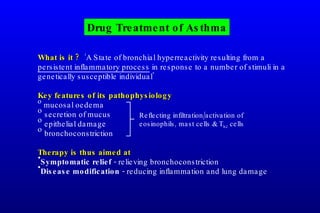
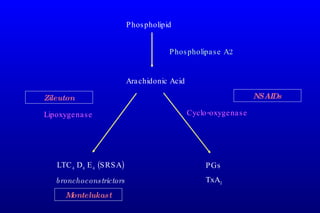
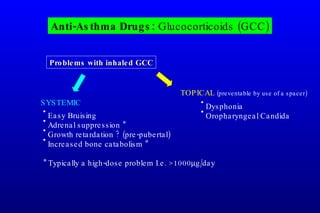
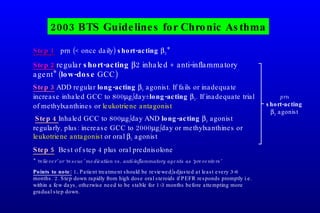
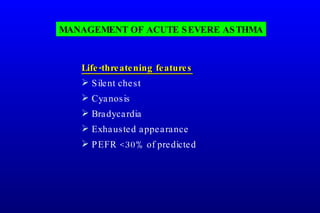
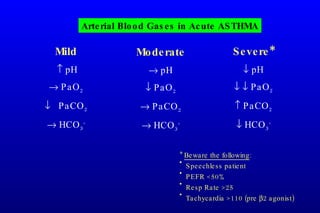
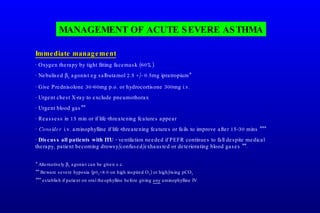
Asthma is a major public health problem affecting over 150 million people worldwide. It is caused by bronchial hyperreactivity and airway inflammation in response to various stimuli in genetically susceptible individuals. Common triggers include allergens, exercise, viral infections, and air pollution. Treatment aims to provide symptomatic relief through bronchodilation and modify the underlying disease process using anti-inflammatory drugs such as inhaled corticosteroids. Acute exacerbations can be life-threatening and require prompt treatment with bronchodilators, systemic corticosteroids, and oxygen supplementation.
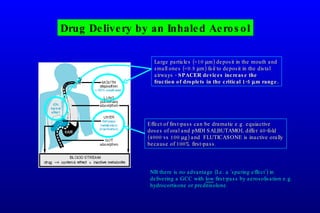
![Drug Delivery Systems: Metered-dose Inhalers MDIs Pressurised MDI (pMDI) CFC (being replaced by HFA) propellant Require co-ordinated activation/inhalation Dry Powder MDI No propellant Require only priming then sucking Low PEFR a problem (<60L/min) Delivery humidity dependent ? Orange [fluticasone] Blue [short acting 2 agonist] Green [salmeterol] Brown [BDP or budesonide] Turbuhaler Diskhaler](https://image.slidesharecdn.com/p3respdrugslecture000-1233730950067181-1/85/Respiratory-Drugs-for-Asthma-COPD-12-320.jpg)







































































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
