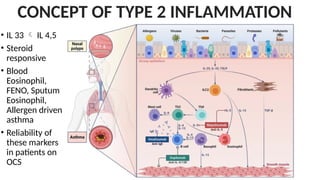
• IL 33 IL 4,5
• Steroid
responsive
• Blood
Eosinophil,
FENO, Sputum
Eosinophil,
Allergen driven
asthma
• Reliability of
these markers
in patients on
OCS
CONCEPT OF TYPE 2 INFLAMMATION
3.
WHEN NO EVIDENCEOF TYPE 2 ?
• Consider other causes
• LAMA
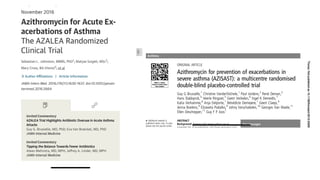
• Low Dose Azithromycin (adults)
• Anti – IL4Ralpha if already on OCS
• Anti thymus Stromal Lymphopoietin ( No Evidence)
5.
TYPE 2 INFLAMMATION
•First Non Biologicals
• Adherence
• Increase dose of ICS
• Treat the conditions like ABPA, Chronic Rhinosinusitis
6.
PREREQUISITES BEFORE STARTING
BIOLOGICALS
1.Should be tried only for patients with severe asthma
2. Only after treatment has been optimized
3. First dose of asthma biologic therapy should not be given on the
same day as a covid vacine
7.
ANTI IG E
•Omalizumab
• Subcutaneous
• Age >6 years
• Eligibility criteria : Sensitization, More exacerbation
8.
Anti IL 5or Anti IL5R
• Mepolizumab or benralizumab
• 4 months
• IV
• Infusion every 4 weeks
9.
REVIEW
• Re evaluateonce every 3-6 months
• Oral drugs, first to decrease or stopping OCS first
• Inhaled treatments, consider reducing the ICS dose after 3-6 months
but do not completely stop inhaled therapy.
• For biologicals, minimum of 12 months of treatment needed. Relapse
after stopping biologicals in RCTs.
10.
EXACERBATIONS
• Exacerbations representan acute or sub-acute worsening in
symptoms and lung functions
• MILD TO MODERATE: Talks in phrases, prefers sitting, RR 16-30, HR
100-120, Spo2 >90 PEF >50 <80
• Severe RR >30, Accessary Muscle usage, PR >120, PEF <50
11.
Clinical Danger signs
•Use of accessory muscles
• Inability to lie supine
• Agitation
• Depressed mental status
• Cyanosis
• Silent chest
12.
Incidence of SevereAsthma
• Prevalence of Severe asthma is children 1.6% and 1.16% in adults
(Indian Data 2020-2021) vs 3.7% (GINA Netherlands Data)
• Non Compliance, Under diagnosing and Stigma
13.
Objective Assessments
• PEFor FEV in Severe Asthma? Spirometry?
• Oxygen Saturation – Spo2 <92% predictor of Hospitalization (Level C)
• FDA has recently issued a safety communication on overestimation of
oxygen saturation in people with dark skin color
14.
PaCo2
• Normal Co2vs Low Co2
• Increased Respiratory drive in acute asthma resulting in
hyperventilation Decreased PC02
• Thus a Normal PCo2 during an exacerbation denotes severe airway
narrowing and dynamic hyperinflation, even tidal volume and alveolar
ventilation are starting to decrease, despite persistent increase in
drive.
• Hypercapnea is not a far fetch from normal PCo2.
15.
• Less roleof Chest Xray, unless strong suspicion of Asthma is ruled out.
BETA AGONISTS
• ShortActing Albuterol or Levalbuterol
• Albuterol 2.5 to 5 mg by Jet nebulization every 20 minutes for three
doses, then 2.5 mg to 5 mg every one to four hours as needed.
• MDI VS NEBULISATION
• CONTINOUS VS INTERMITTENT
19.
SYSTEMIC CORTICOSTEROIDS
• LevelA Evidence
• Should be administered within 1 hour of presentation
• 1mg/Kg
• No benefit in tapering the dose after 5 days
20.
ICS
HIGHLY RECOMMENDED ALONGWITH ADMINISTRATION OF SCS
MAINTENENANCE AND RELEIVER THERAPY WITH ICS-FORMETEROL
REDUCED EXACERBATION BY 32%
21.
IPRATROPIUM BROMIDE
• LEVELA Evidence in adults and B in children
• Only nausea and tremors were reduced in children
MAGNESIUM
• IV MGSO4NOT RECOMMENDED IN ACUTE EACERBATION
• But single dose 2g administration decreased rates of hospital
admission even in people with Low FEV1 (Evidence Level A)
• But clearly no role of Nebulized Magnesium
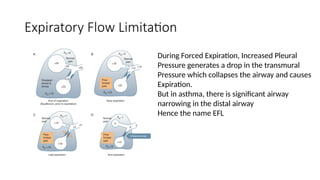
Expiratory Flow Limitation
DuringForced Expiration, Increased Pleural
Pressure generates a drop in the transmural
Pressure which collapses the airway and causes
Expiration.
But in asthma, there is significant airway
narrowing in the distal airway
Hence the name EFL
ROLE OF NIV
•Controversial
• Cochrane Review 2012 - Inconclusive
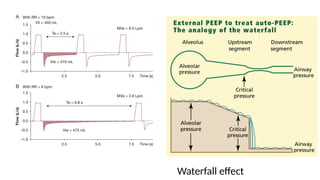
• Cons: Dynamic Hyperinflation if Ext PEEP >> iPEEP
• Increased risk of barotrauma
• Incorrect Patient selection
• BiPAP settings PEEP at 3-5, iPAP 7-15, RR<25, high inspiratory flow
rate, low I:E ratio
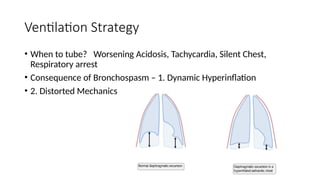
Strategy in MechanicalVentilation
• Use the largest tube possible
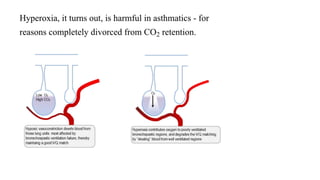
• Avoid Hyperoxia as target spo2 >95 results in V/Q Mismatch
• Small Tidal Volume to avoid DHI
• High Inspiratory flow
• More time for Expiration
• Ignore the High Peak Airway pressure alarms or change the limit
• Use heavy sedation