Downloaded 223 times
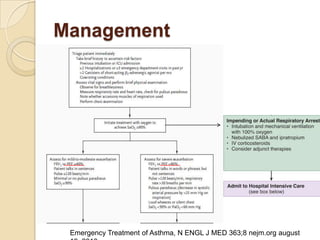
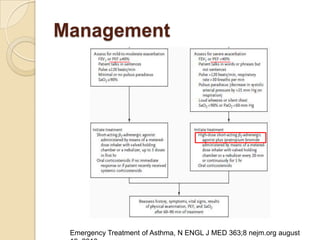
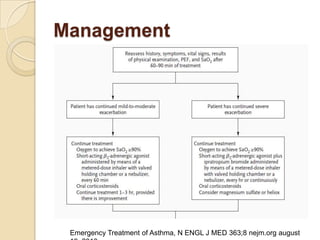
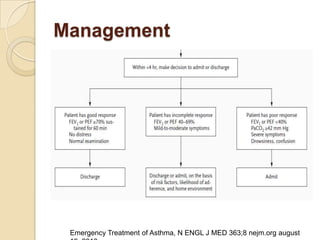
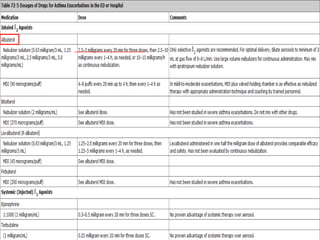
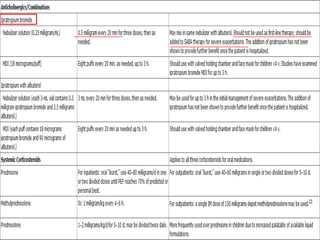
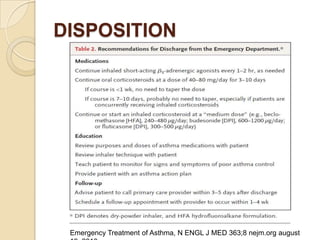


Acute asthma exacerbations are characterized by bronchospasm and airway inflammation. Key goals in treatment are rapid reversal of airflow obstruction through repetitive administration of inhaled short-acting beta-2 agonists and ensuring adequate oxygenation. Systemic corticosteroids improve resolution of obstruction and reduce relapse rates. Inhaled corticosteroids are also beneficial when combined with short-acting beta-2 agonists. Anticholinergic agents and intravenous beta-2 agonists may be considered for severe exacerbations unresponsive to other therapies.
























































![Microsoft+PowerPoint+-+Asthma+4th+year+Lecture+(1)+[Compatibility+Mode].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/microsoftpowerpoint-asthma4thyearlecture1compatibilitymode-230704125445-487a63ed-thumbnail.jpg?width=640&height=640&fit=bounds)





















