Downloaded 76 times
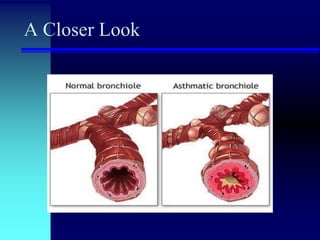

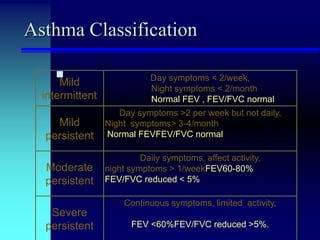






Asthma is a chronic inflammatory disorder of the airways characterized by variable airflow obstruction and airway hyperresponsiveness. It has different classifications based on severity and is treated through long-term control medications like inhaled corticosteroids and bronchodilators as well as quick-relief medications for acute symptoms. The pathophysiology involves airway inflammation, remodeling, and hyperresponsiveness triggered by allergens, infections, and other environmental factors.

























































![Microsoft+PowerPoint+-+Asthma+4th+year+Lecture+(1)+[Compatibility+Mode].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/microsoftpowerpoint-asthma4thyearlecture1compatibilitymode-230704125445-487a63ed-thumbnail.jpg?width=640&height=640&fit=bounds)







![Microsoft PowerPoint - Asthma 4th year Lecture (1) [Compatibility Mode].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/microsoftpowerpoint-asthma4thyearlecture1compatibilitymode-220716165932-01cf3f8c-thumbnail.jpg?width=640&height=640&fit=bounds)



















