Downloaded 318 times














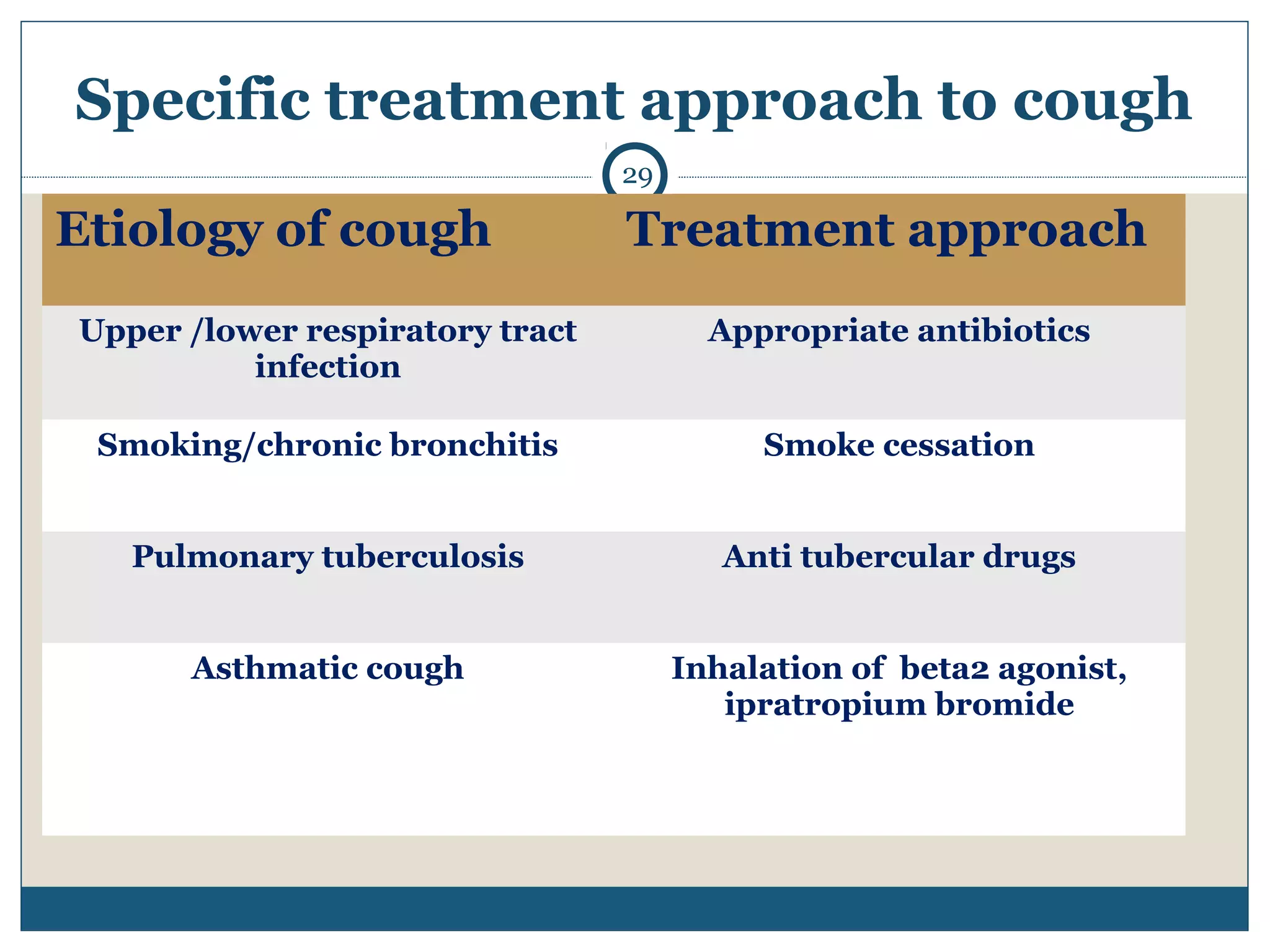



This document discusses drugs used to treat cough. It begins by defining cough and classifying it based on duration and characteristics. Nonspecific therapies for cough include demulcents to soothe the throat, expectorants to enhance mucus secretion or reduce viscosity, and antitussives to suppress the cough center. Demulcents include lozenges and cough drops. Expectorants include bronchial secretagogues like guaifenesin and mucolytics like bromhexine that break down mucus. Antitussives include opioids like codeine, nonopioids like dextromethorphan, and antihistamines. Specific treatments depend on the underlying cause of cough such as antibiotics for infection






















































































