Downloaded 27 times

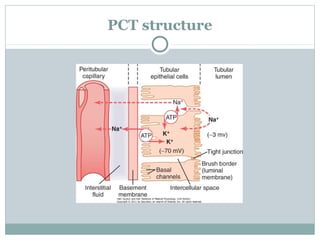
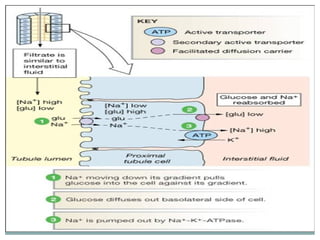
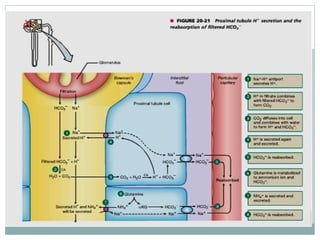

The document summarizes key processes in the nephron including reabsorption and secretion. It describes how different parts of the nephron (proximal convoluted tubule, loops of Henle, distal convoluted tubule) reabsorb various filtrate components like sodium, glucose, water, and change the filtrate composition through secondary active transport and countercurrent mechanisms. It also discusses hormone actions including aldosterone and ADH that regulate sodium and water reabsorption respectively in the collecting ducts.




















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)













