Downloaded 52 times

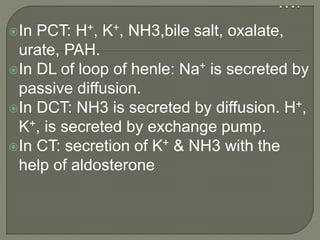
![ If [H+]↑→ Resp. centre stimulated
→hyperventilation→↑volatile acid
excretion.
If [H+]↓→hypoventilation→↑volatile acid
retention](https://image.slidesharecdn.com/renaltasnim-170809190416/85/urine-formation-mechanism-acidification-urinary-buffers-by-dr-Tasnim-53-320.jpg)
![ Buffer system of the body fluid-
1st line of defense
• immediately combines with acid / bases to prevent
marked change of [H+]
• works within a fraction of second to minimize the
changes
• do not eliminate H+ from the body but only keep them
tied up until balanced re-established](https://image.slidesharecdn.com/renaltasnim-170809190416/85/urine-formation-mechanism-acidification-urinary-buffers-by-dr-Tasnim-55-320.jpg)
![ Respiratory system-
2nd line of defense
• respiratory centre regulate the removal of CO2 &
therefore H2CO3 from the body.
• works within a few minutes.
Kidney system-
3rd line of defense
• can excrete either acidic or alkaline urine to maintain
ECF [H+]
• works over a period of hours to several days but it is the
most powerful acid –base regulatory systems.](https://image.slidesharecdn.com/renaltasnim-170809190416/85/urine-formation-mechanism-acidification-urinary-buffers-by-dr-Tasnim-56-320.jpg)


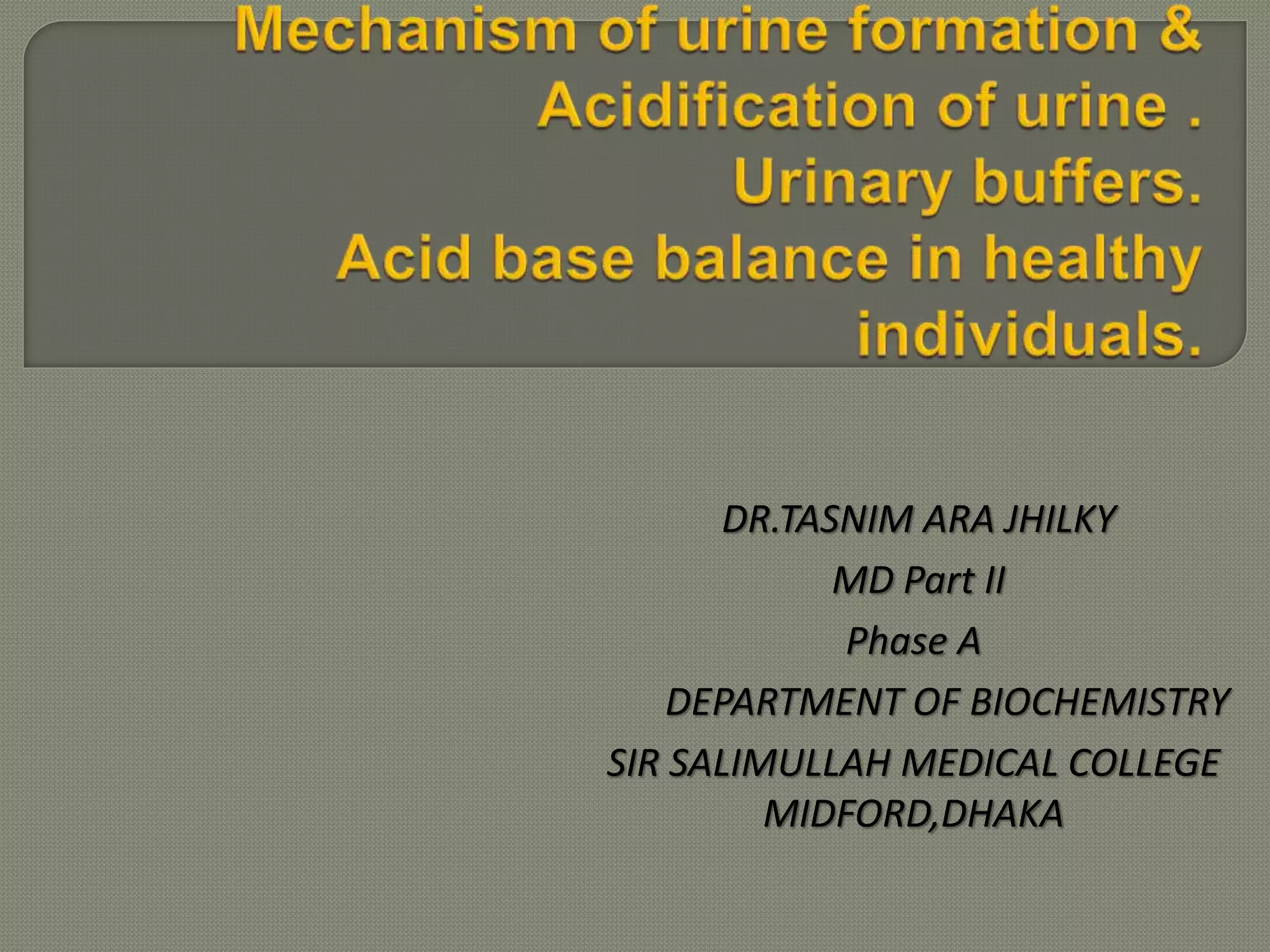
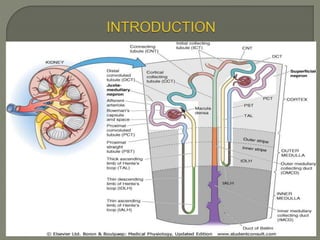
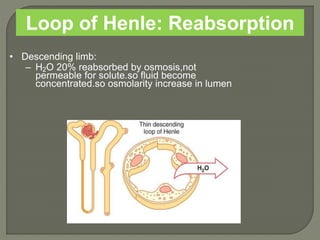
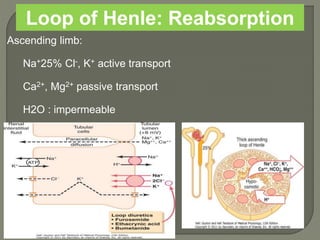
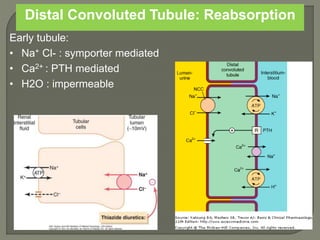
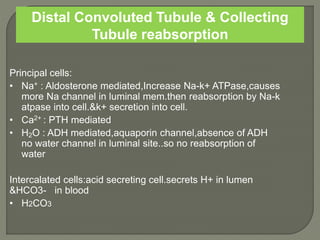
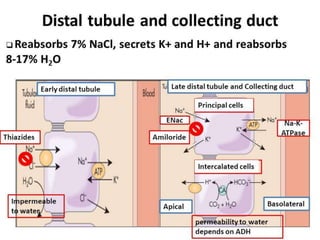
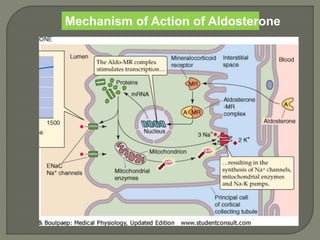
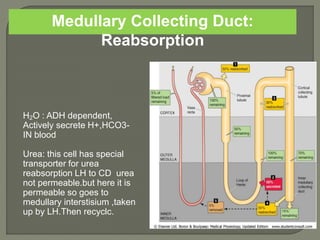
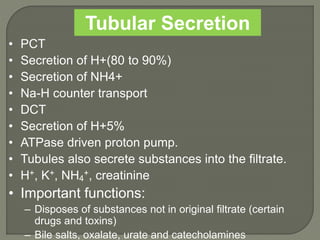
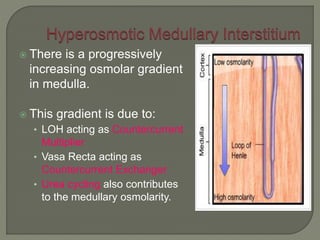
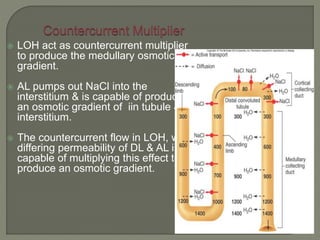
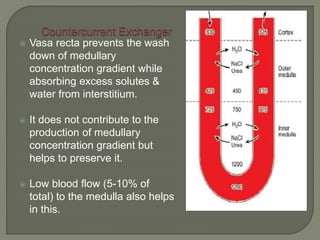
The document discusses the key processes involved in urine formation - glomerular filtration, tubular reabsorption and tubular secretion. It describes the anatomy of nephron segments including the proximal convoluted tubule, loop of Henle and distal convoluted tubule. The mechanisms of reabsorption and secretion in different segments are explained. The role of countercurrent multiplier and exchanger in medullary concentration gradient formation is also summarized.










































![Renal Physiology. [Compatibility Mode].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/renalphysiology-250924082023-9109186b-thumbnail.jpg?width=640&height=640&fit=bounds)




































