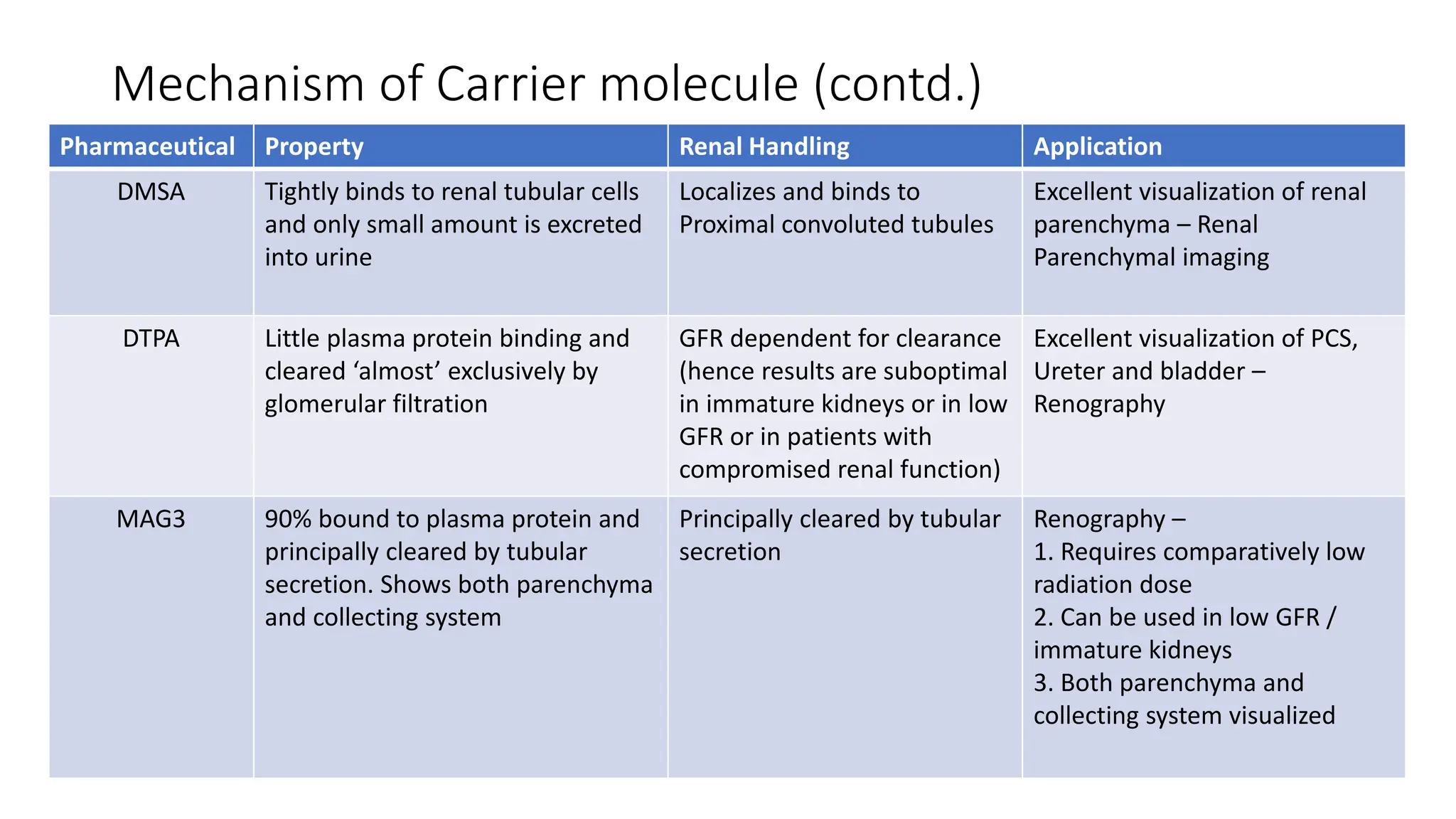
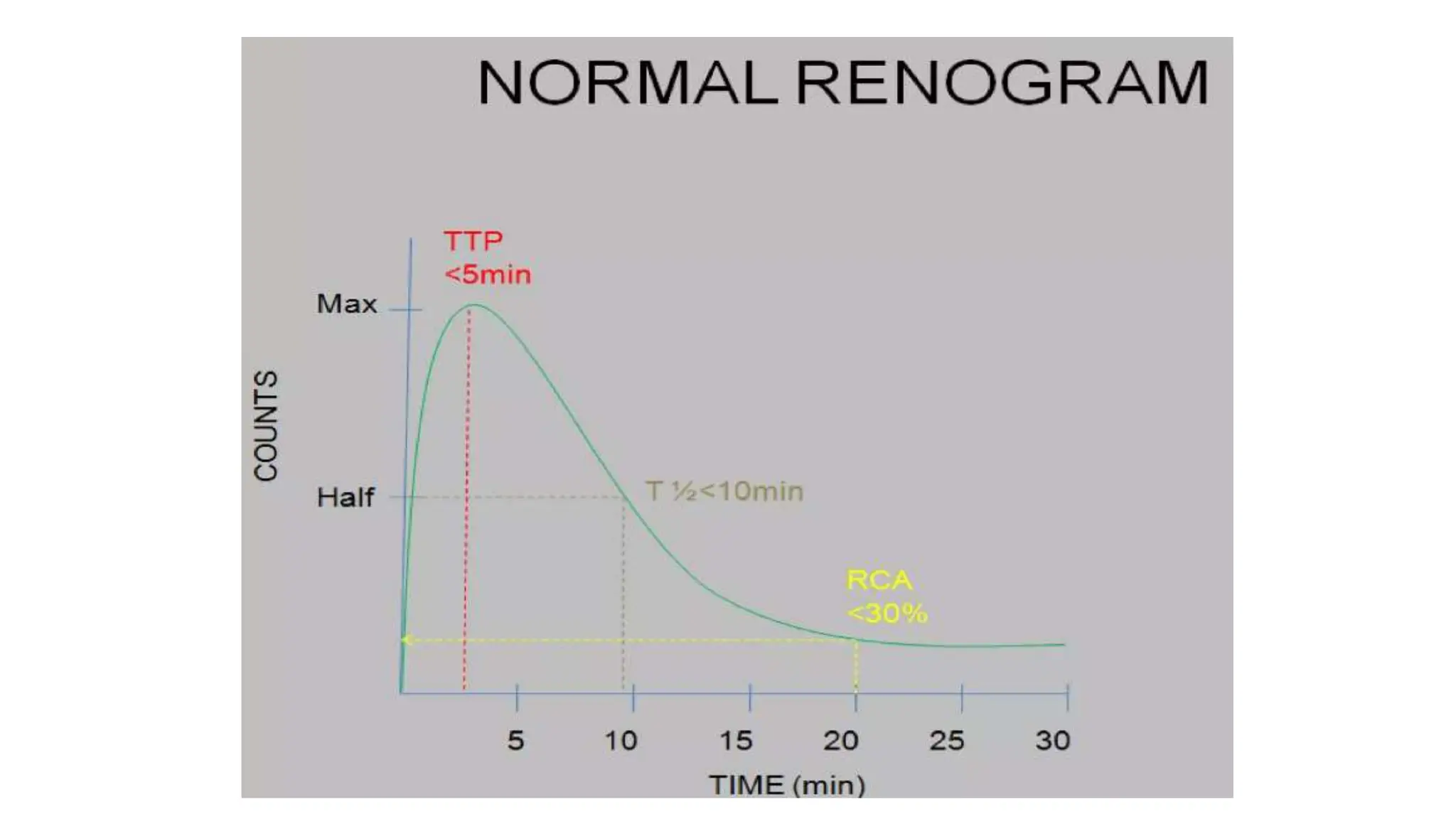
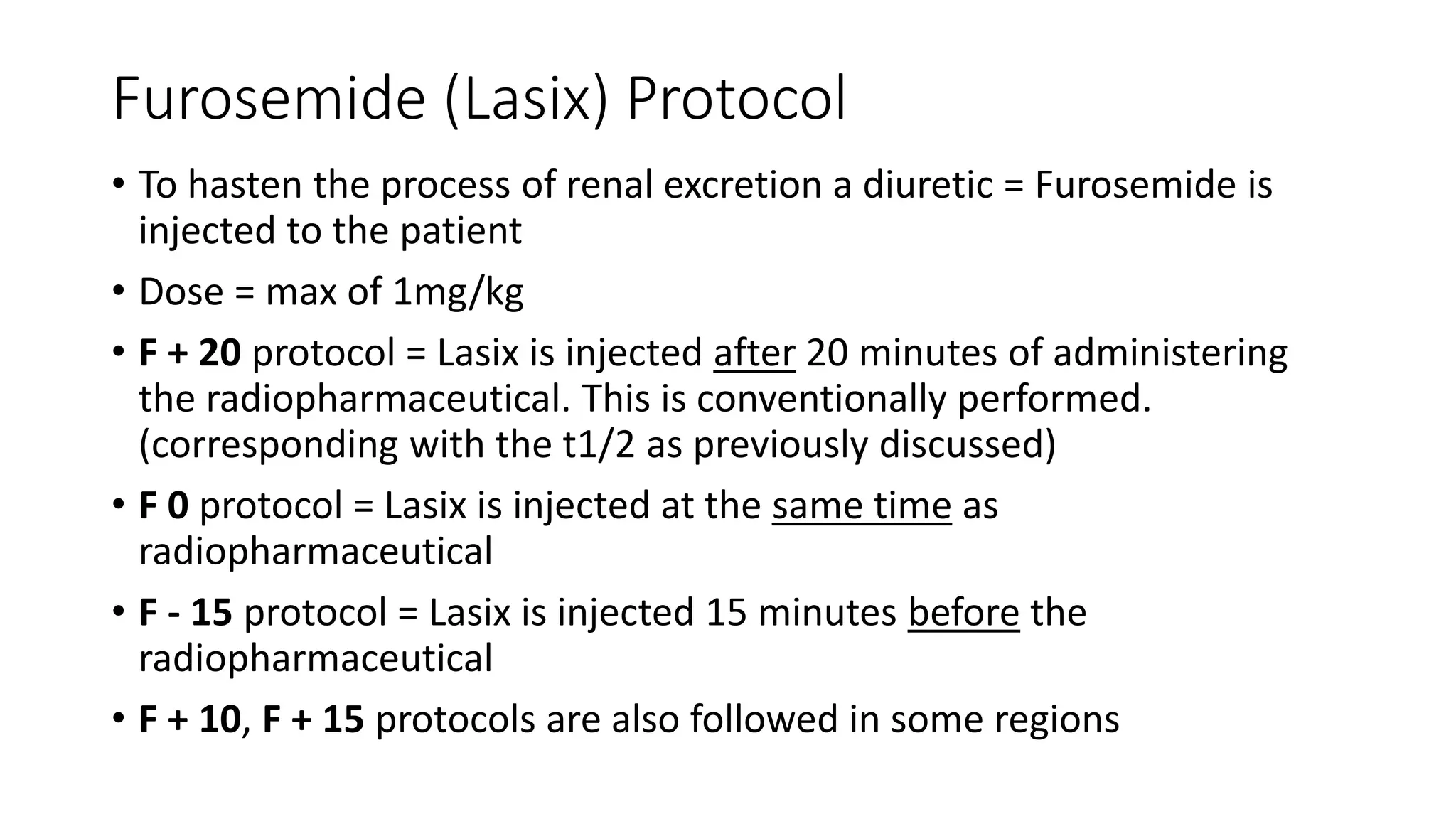
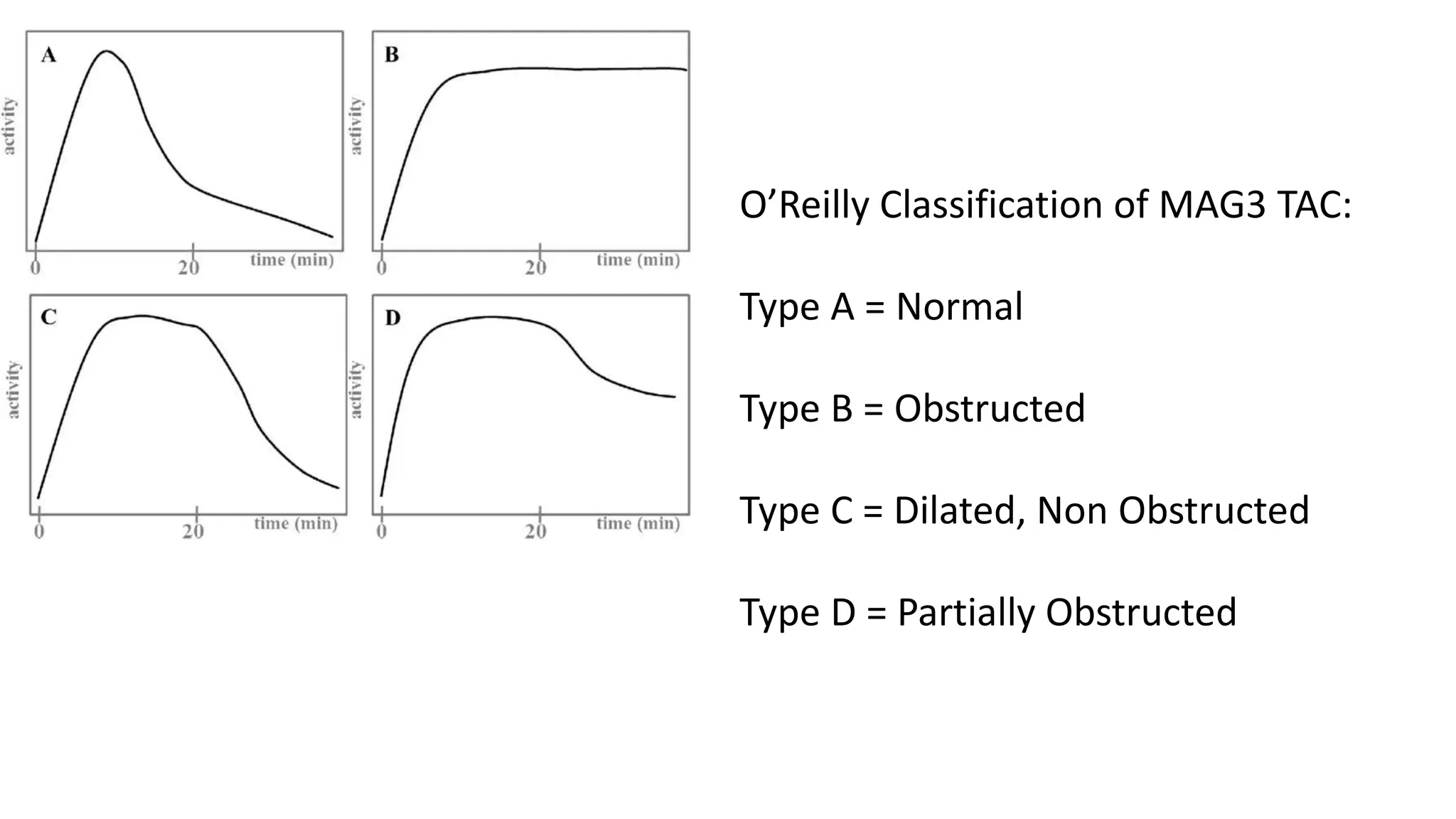
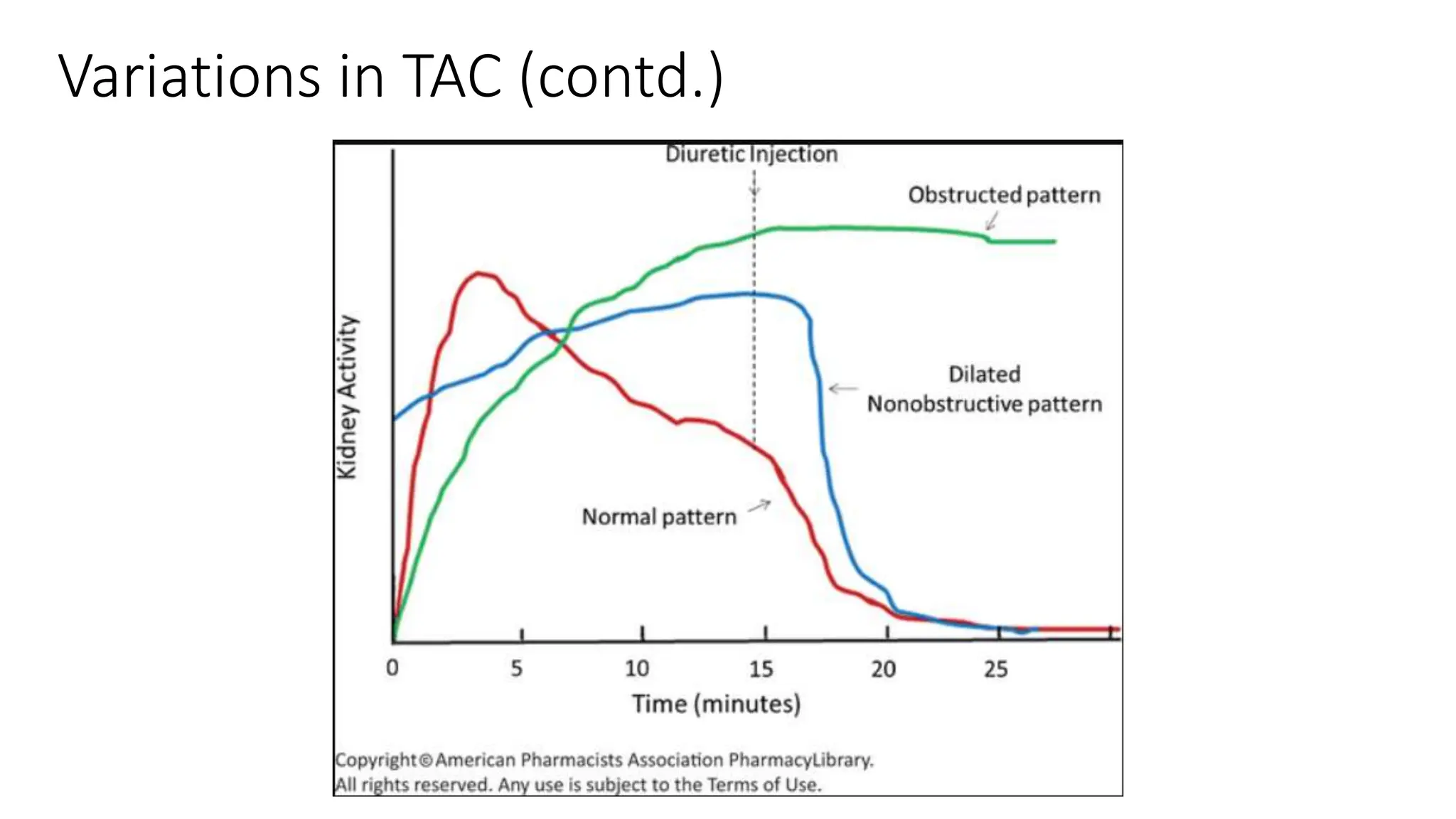
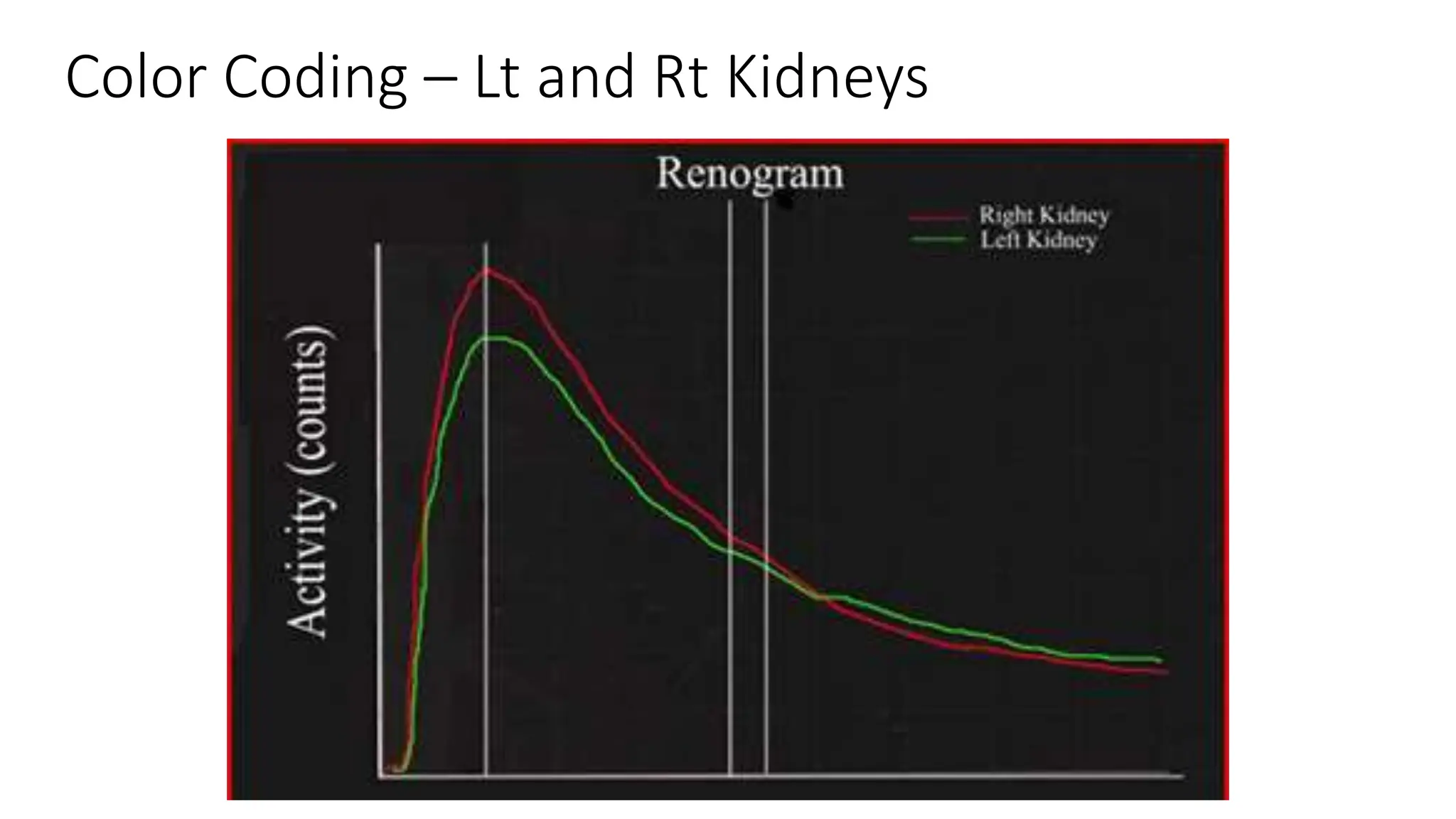
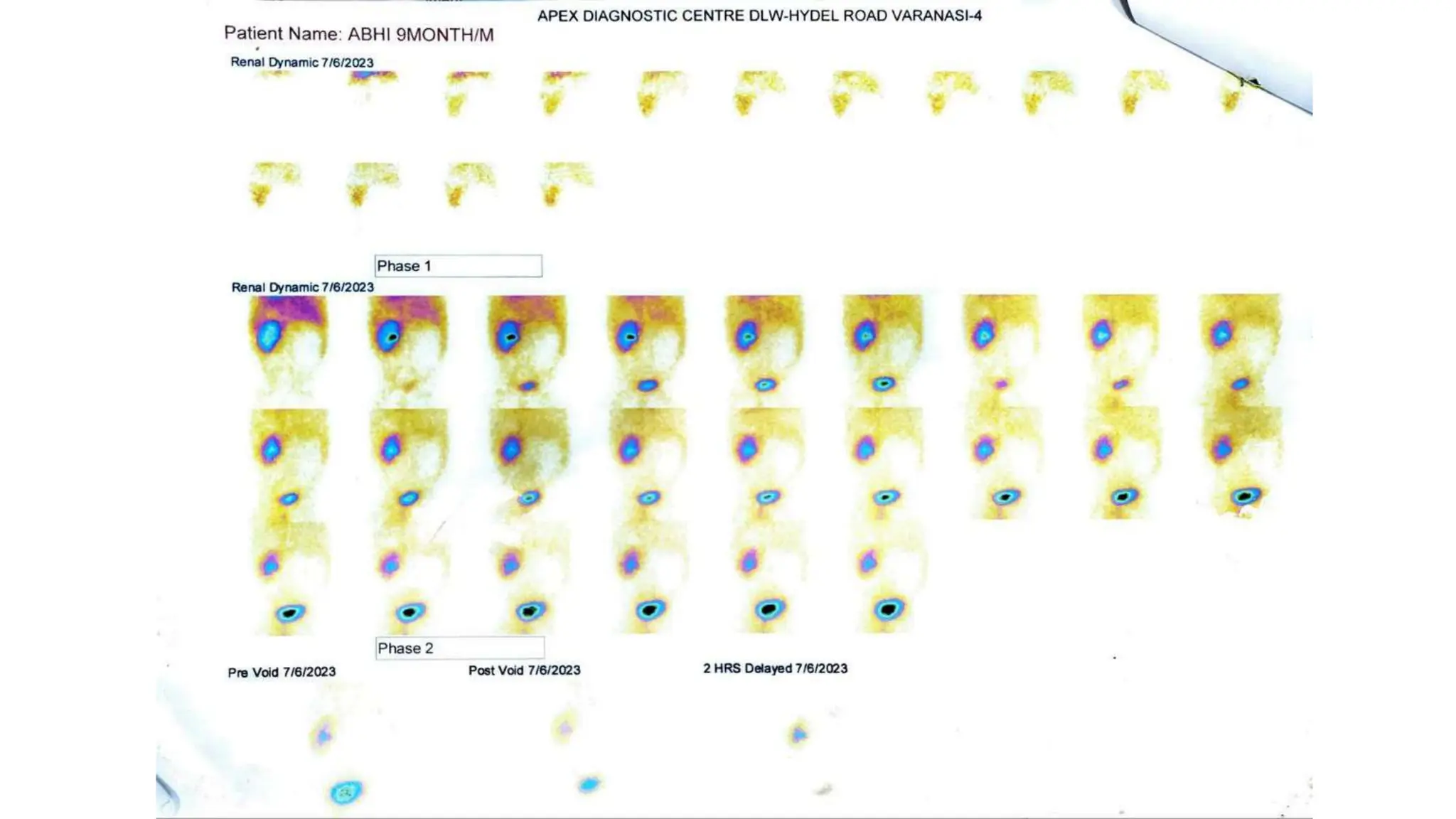
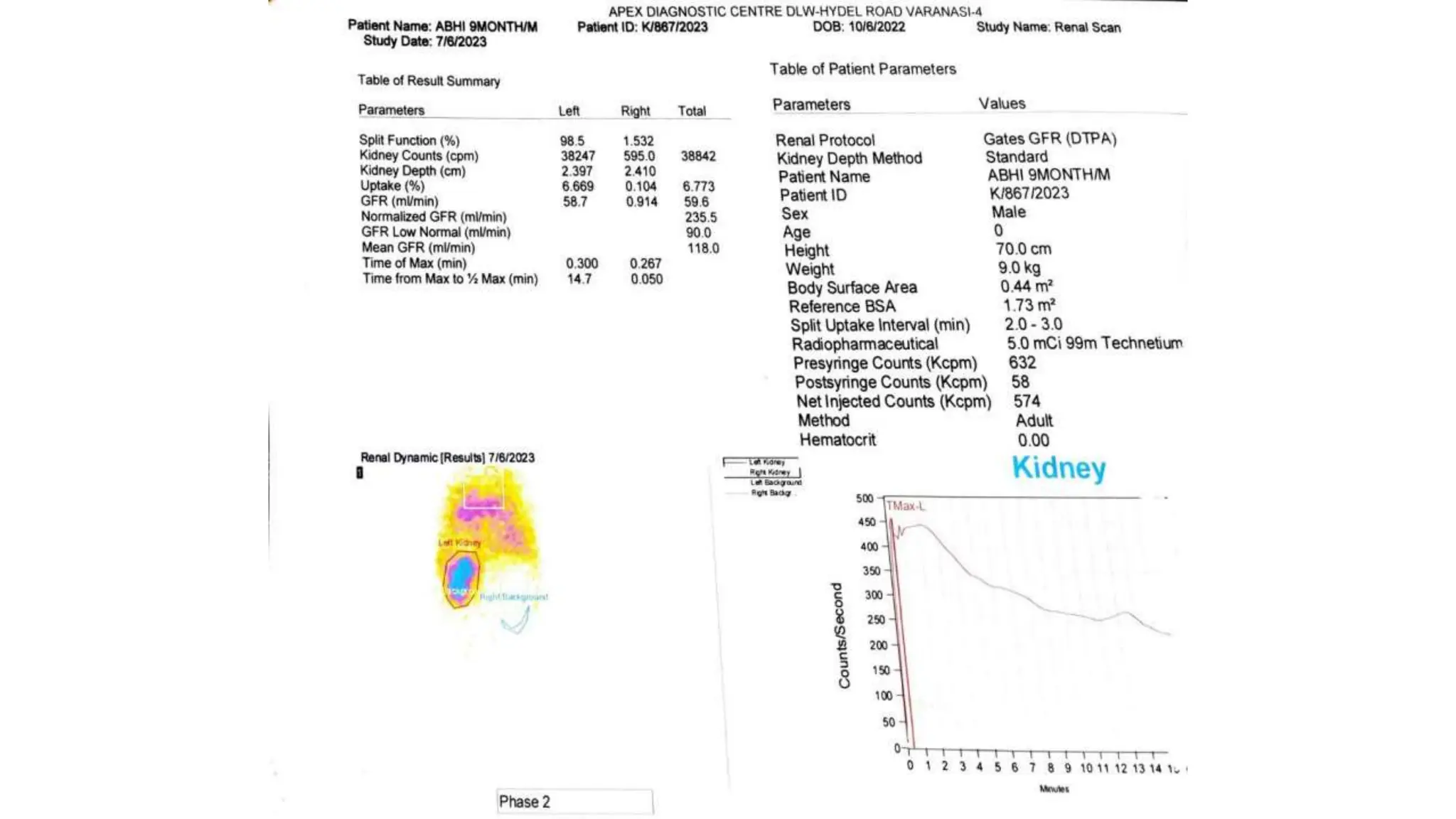
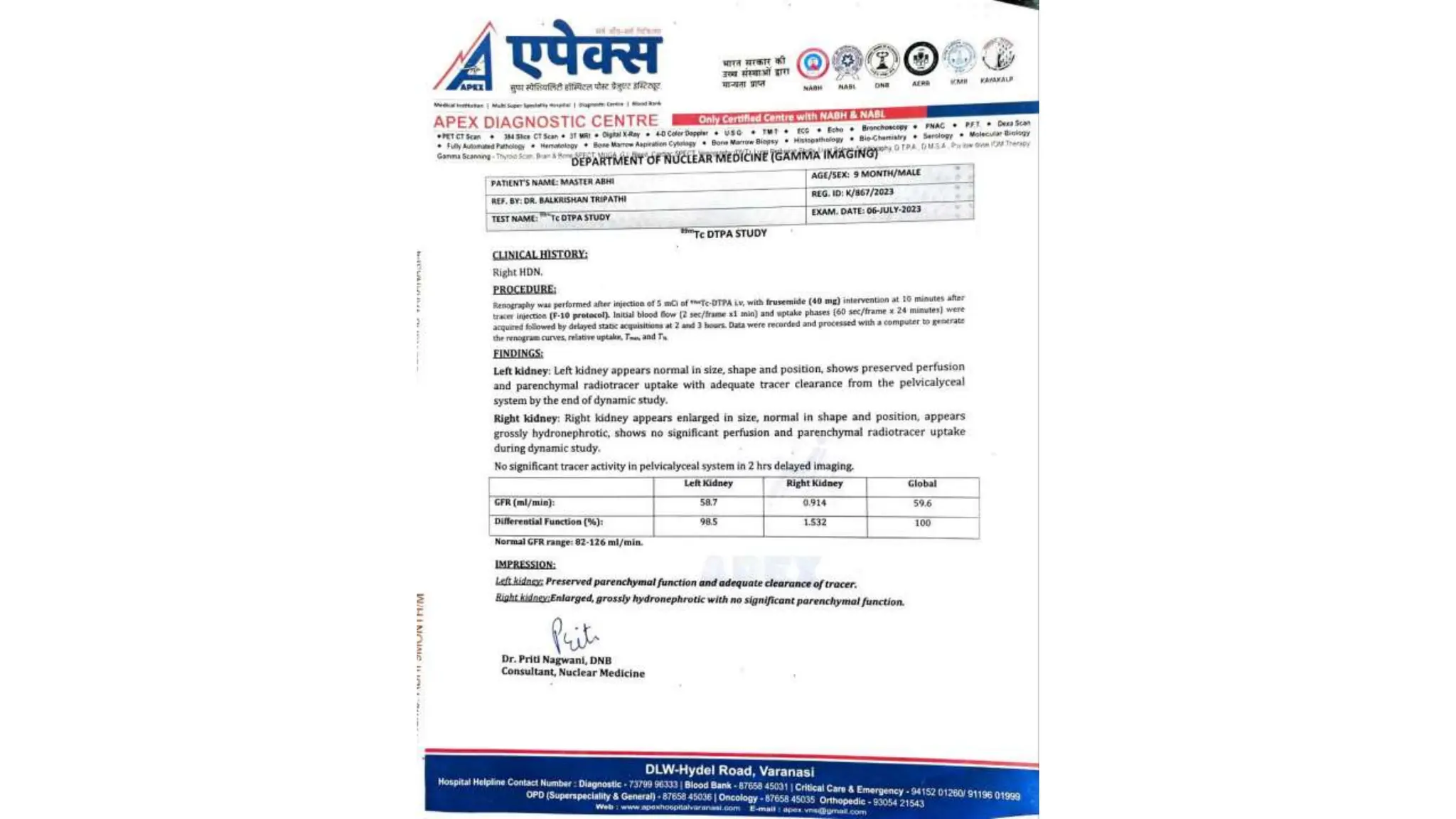
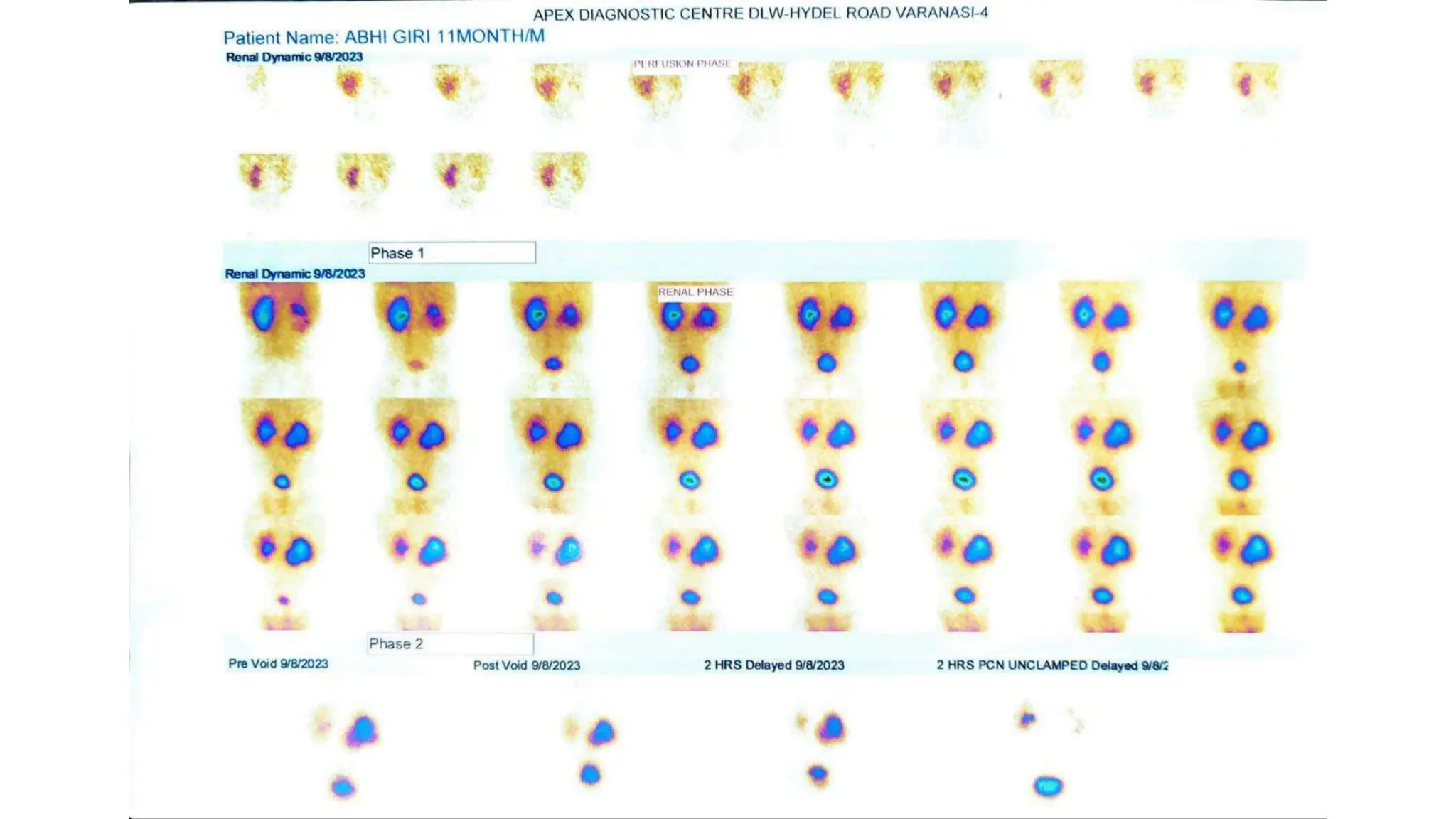
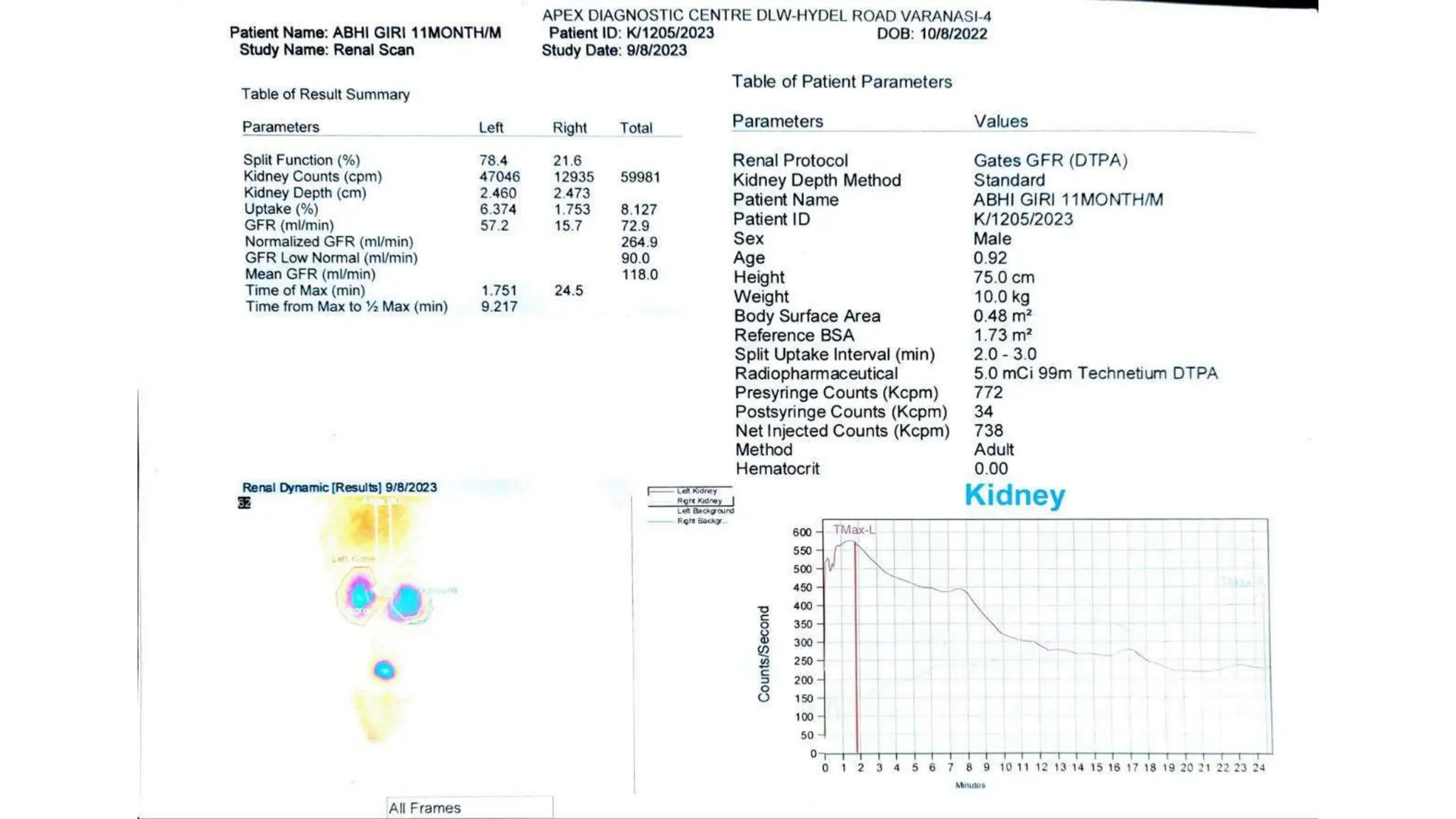
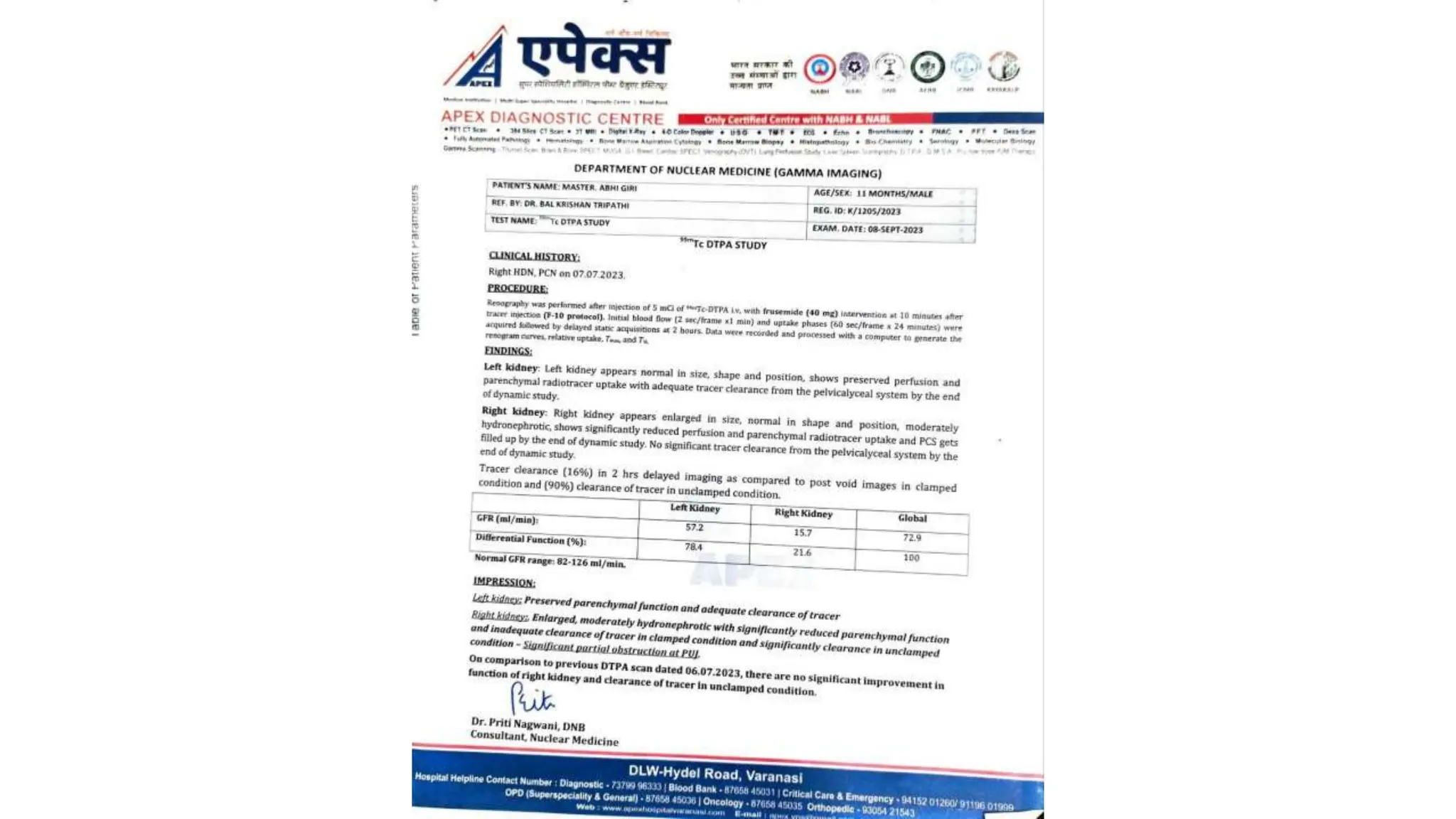
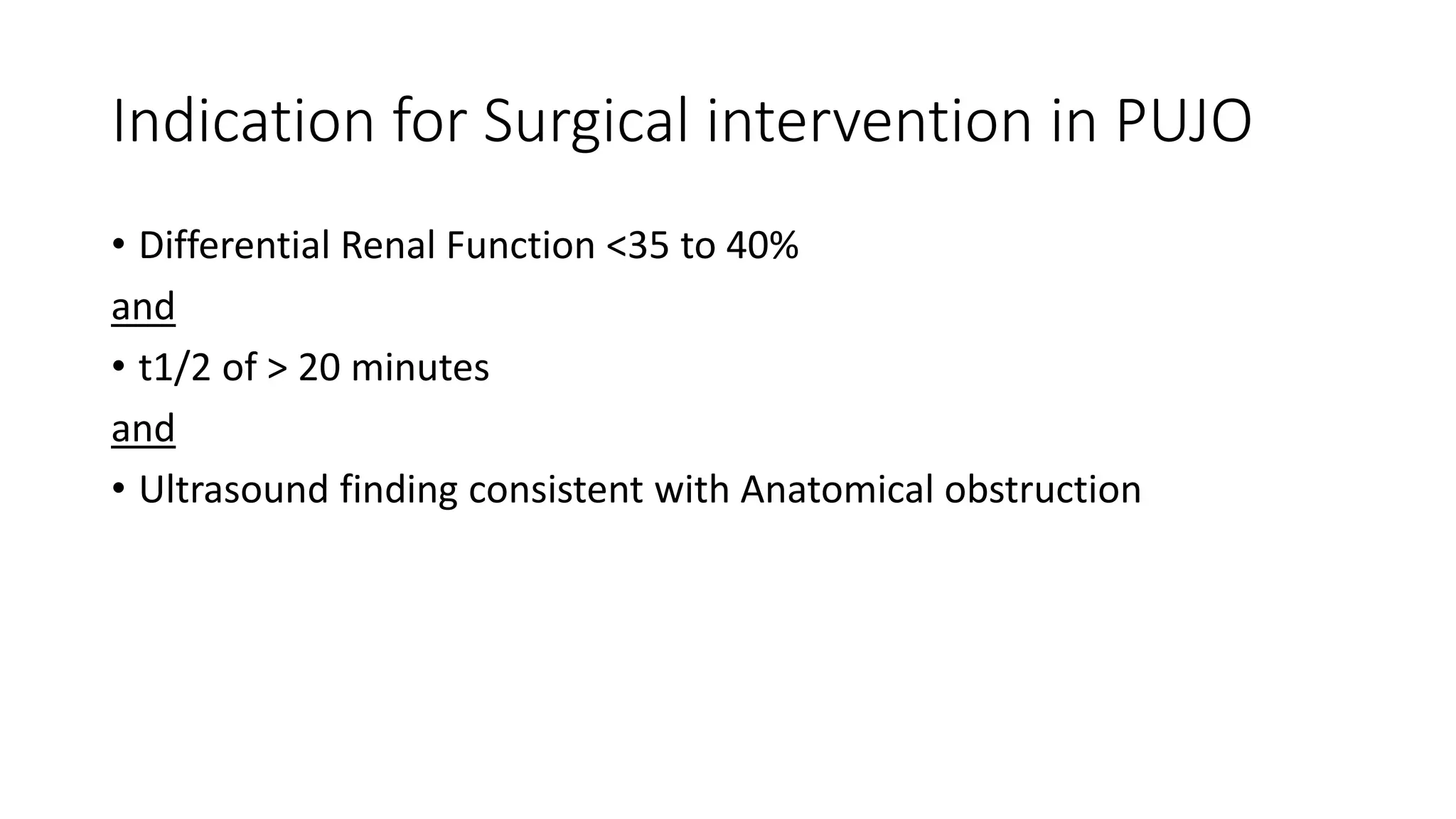
This document summarizes the renal isotope scan procedure. It discusses how radiopharmaceuticals like DMSA, DTPA, and MAG3 are used to evaluate renal function and anatomy. The scan involves injection of the radiopharmaceutical followed by imaging in three phases - perfusion, parenchymal, and excretory. Parameters like time to peak, half-life, residual cortical activity, and differential renal function are analyzed. The document presents examples of normal and abnormal renogram curves and how they indicate conditions like obstruction. It outlines the procedure, roles of diuretics, and indications for surgery in pediatric urinary obstruction cases.