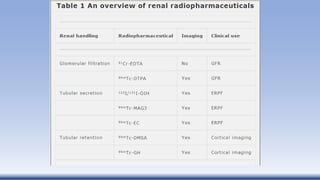
This document discusses the use of radionuclides in urology imaging. It begins by providing a brief history of radionuclides and nuclear medicine. It then describes various radionuclides used for imaging and therapy, as well as their desirable characteristics. Common radiopharmaceutical agents like Tc-99m MAG3 and DMSA are discussed. Basic renal scan protocols and various renal imaging techniques including renography and quantification of renal function are summarized. Indications and protocols for diuretic renal scans and renal cortical scintigraphy are also provided.