Downloaded 218 times
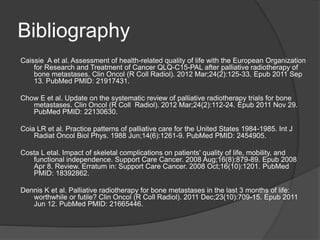
![Trivia: Bone Mets
Response to radiotherapy is not related to
severity of pretreatment pain
[Kirou‐Mauro A et al. Int J Radiat Oncol Biol Phys
2008;71:1208‐1212]
Pain flare occurs in 10‐25% of patients treated
with radiotherapy (1‐2 days post‐treatment);
readily controlled/prophylaxed with steroids
[Hird A et al. Clin Oncol 2009;21:329‐335. Hird A et al. Int J Radiat
Oncol Biol Phys 2009]
QOL improves after radiotherapy for bone mets
(pain, anxiety, sense of well‐being)
[Chow E et al. Support Cancer Ther 2004;1:179‐184]](https://image.slidesharecdn.com/radiationtherapyinpalliativecare2012-120322163323-phpapp01/85/Radiation-Therapy-in-Palliative-Care-Spring-2012-31-320.jpg)
![Bibliography - continued
George R et al. Interventions for the treatment of metastatic extradural spinal cord
compression in adults. Cochrane Database Syst Rev. 2008 Oct 8;(4):CD006716.
Review. PubMed PMID: 18843728.
Hashimoto K et al. Palliative radiation therapy for hemorrhage of unresectable gastric
cancer: a single institute experience. J Cancer Res Clin Oncol. 2009 Aug;135(8):1117-
23. Epub 2009 Feb 10. PubMed PMID: 19205735.
Higginson DS et al.Predicting the need for palliative thoracic radiation after first-line
chemotherapy for advanced nonsmall cell lung carcinoma. Cancer. 2011 Sep 20.
doi:10.1002/cncr.26495. [Epub ahead of print] PubMed PMID: 21935913.
Kim MM et al. Clinical benefit of palliative radiation therapy in advanced gastric cancer.
Acta Oncol. 2008;47(3):421-7. PubMed PMID: 17899453.](https://image.slidesharecdn.com/radiationtherapyinpalliativecare2012-120322163323-phpapp01/85/Radiation-Therapy-in-Palliative-Care-Spring-2012-43-320.jpg)
![Bibliography - Continued
Lester JF, Macbeth FR, Toy E, Coles B. Palliative radiotherapy regimens for non-small cell
lung cancer. Cochrane Database Syst Rev. 2006 Oct 18;(4):CD002143. Review.
PubMed PMID: 17054152.
Lester JF, Macbeth FR, Brewster AE, Court JB, Iqbal N. CT-planned accelerated
hypofractionated radiotherapy in the radical treatment of non-small cell lung cancer.
Lung Cancer. 2004 Aug;45(2):237-42. PubMed PMID: 15246196.
Loblaw DA, Mitera G, Ford M, Laperriere NJ. A 2011 Updated Systematic Review and
Clinical Practice Guideline for the Management of Malignant Extradural Spinal Cord
Compression. Int J Radiat Oncol Biol Phys. 2012 Mar 13. [Epub ahead of print]
PubMed PMID: 22420969.
Lutz S, Korytko T, Nguyen J, Khan L, Chow E, Corn B. Palliative radiotherapy: when is it
worth it and when is it not? Cancer J. 2010 Sep-Oct;16(5):473-82. Review. PubMed
PMID: 20890143.](https://image.slidesharecdn.com/radiationtherapyinpalliativecare2012-120322163323-phpapp01/85/Radiation-Therapy-in-Palliative-Care-Spring-2012-44-320.jpg)

This document provides an overview of palliative radiation therapy for cancer patients. It discusses the fundamentals of how radiation works and advances that have allowed it to more effectively treat cancer. It then focuses on how palliative radiation can effectively relieve symptoms from bone metastases, lung cancer, bleeding, and other cancers in 1-3 fractions rather than longer courses of treatment. Studies show short fractionation schedules provide pain relief comparable to longer schedules with fewer side effects and greater convenience. The document provides guidance on discussing palliative radiation options with radiation oncologists to help simplify the process for hospice patients.















![Rrecent advances in linear accelerators [MR linac]](https://cdn.slidesharecdn.com/ss_thumbnails/icroproadvance2021-recentadvancesinlinearaccelerators-211201040416-thumbnail.jpg?width=640&height=640&fit=bounds)


















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)








