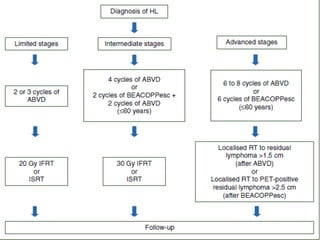
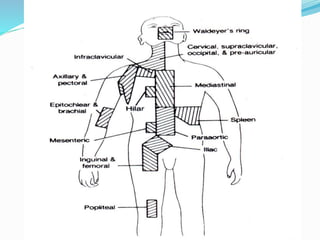
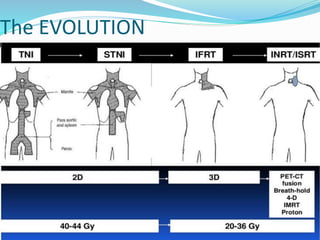
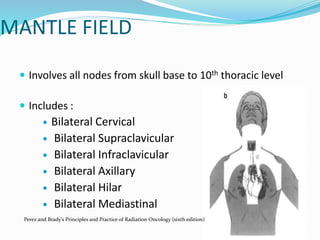
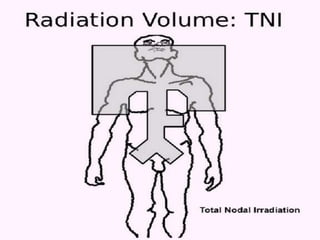
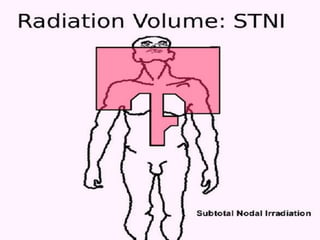
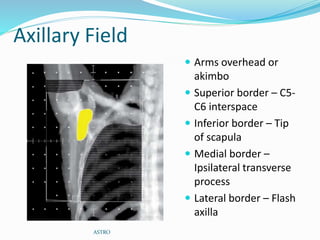
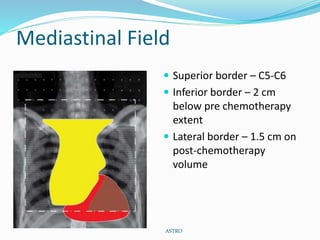
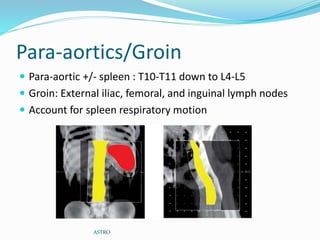
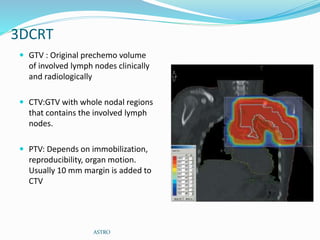
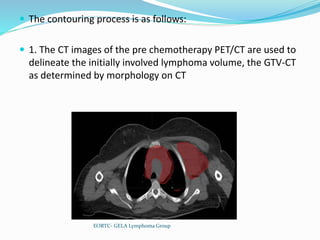
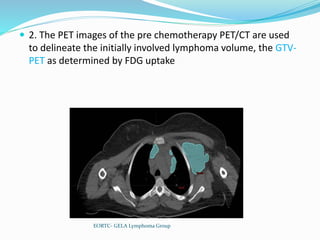
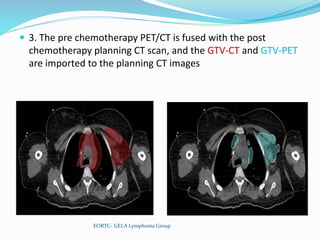
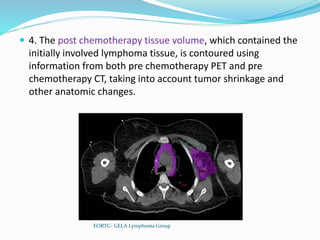
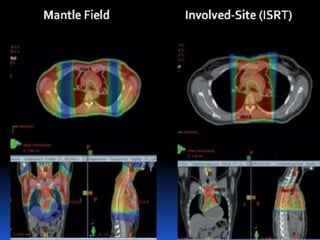
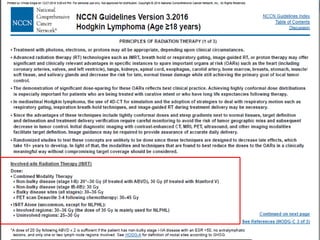
Radiotherapy is used as primary treatment for early-stage Hodgkin lymphoma or as part of combined modality treatment with chemotherapy. Historically, large mantle fields covering lymph node regions from the skull to the pelvis were used. More modern approaches use smaller involved field radiotherapy targeting only initially involved lymph node regions after chemotherapy based on imaging. Proper delineation of clinical target volumes requires pre-chemotherapy imaging ideally with PET/CT to define original disease extent.